NAD+ IV therapy is an intravenous treatment that delivers nicotinamide adenine dinucleotide directly into the bloodstream to restore cellular levels of this essential coenzyme. NAD+ drives mitochondrial energy production, DNA repair, and sirtuin activation in every living cell, yet its levels decline progressively with age.
We cover the science behind NAD+ and age-related depletion, how IV delivery works and what sessions involve, proven therapeutic benefits, ideal candidate profiles, treatment expectations and frequency, cost considerations, safety and research status, comparisons to oral supplements, and how mobile services improve accessibility.
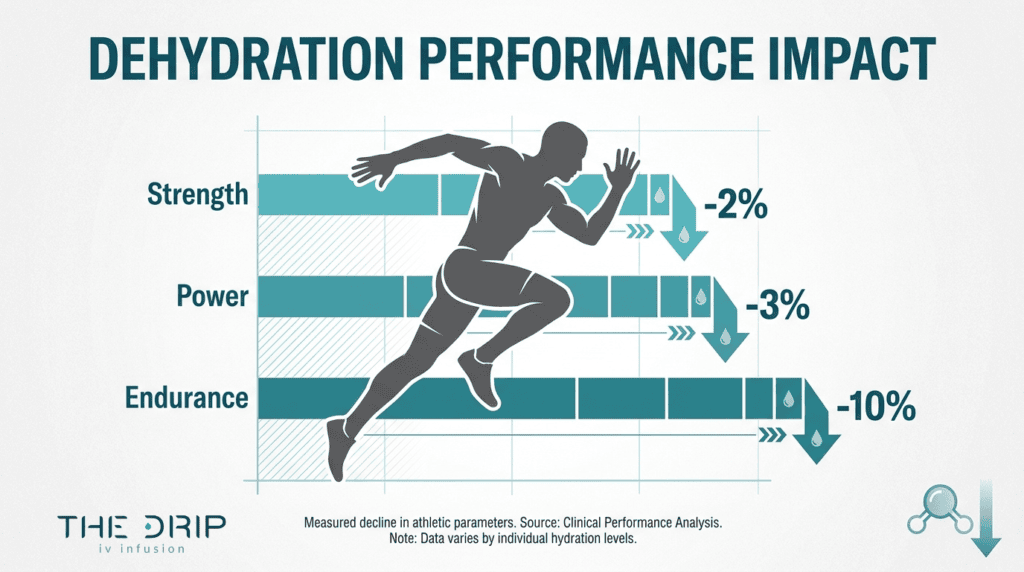
NAD+ functions as an electron carrier in ATP production and a substrate for PARP enzymes and sirtuins. Brain levels decline 10% to 25% between young adulthood and old age, triggering fatigue, cognitive decline, and accelerated aging when stores run critically low.
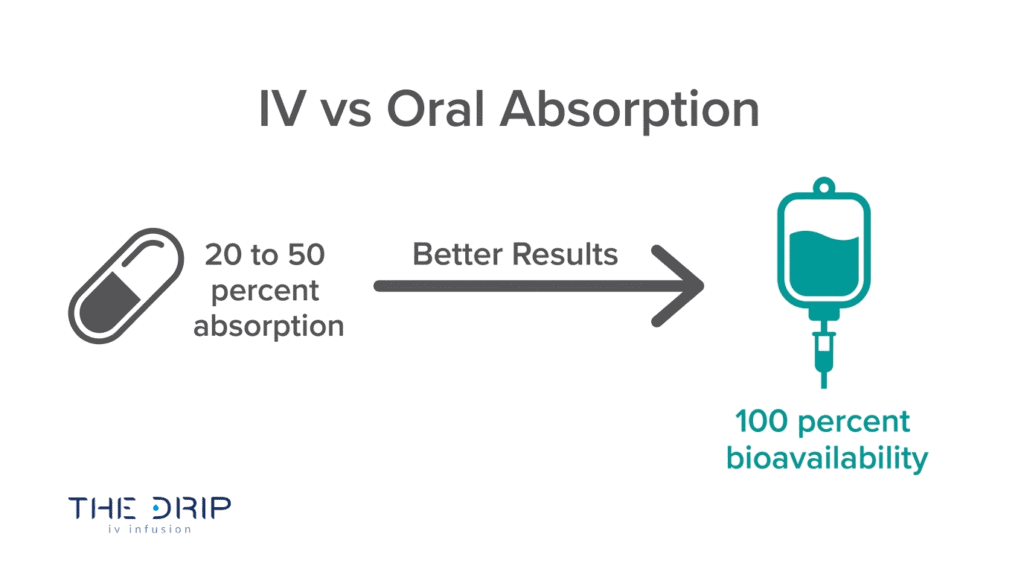
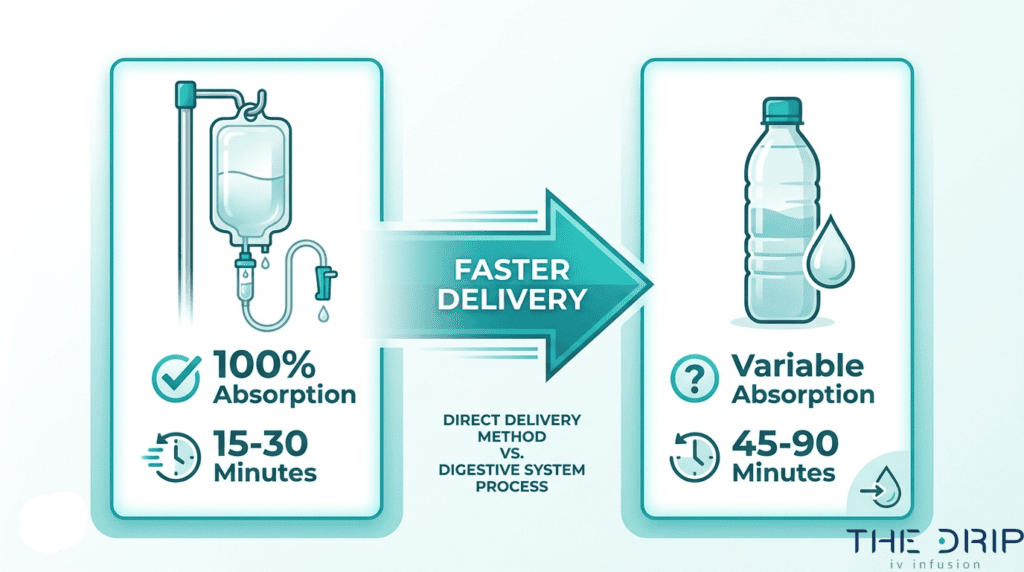
Intravenous delivery achieves near 100% bioavailability by bypassing digestive breakdown and liver metabolism. Sessions last 2 to 4 hours at dosages between 250 mg and 1,000 mg, with infusion rates kept slow to minimize temporary side effects like nausea or chest tightness.
Clinical evidence supports benefits spanning cognitive restoration through reduced neuroinflammation, decreased substance cravings and anxiety in addiction recovery, lower inflammatory markers like CRP and cytokines, and enhanced cellular energy output. Athletic recovery also improves, though direct performance gains in healthy young individuals remain unproven.
Primary candidates include adults over 40 experiencing chronic fatigue, brain fog, or visible aging signs, along with athletes seeking faster recovery between training sessions.
Compared to oral NMN, NR supplements, and nasal sprays, IV therapy produces the highest immediate plasma concentrations with the fewest conversion steps. Mobile delivery through The Drip IV Infusion eliminates clinic visits, making multi-hour sessions practical in your own environment.
What Is NAD+ and Why Is It Important for Your Body?
NAD+ is important for your body because it drives cellular energy production, DNA repair, and longevity pathways. The following sections explain its biological role, age-related decline, and consequences of deficiency.
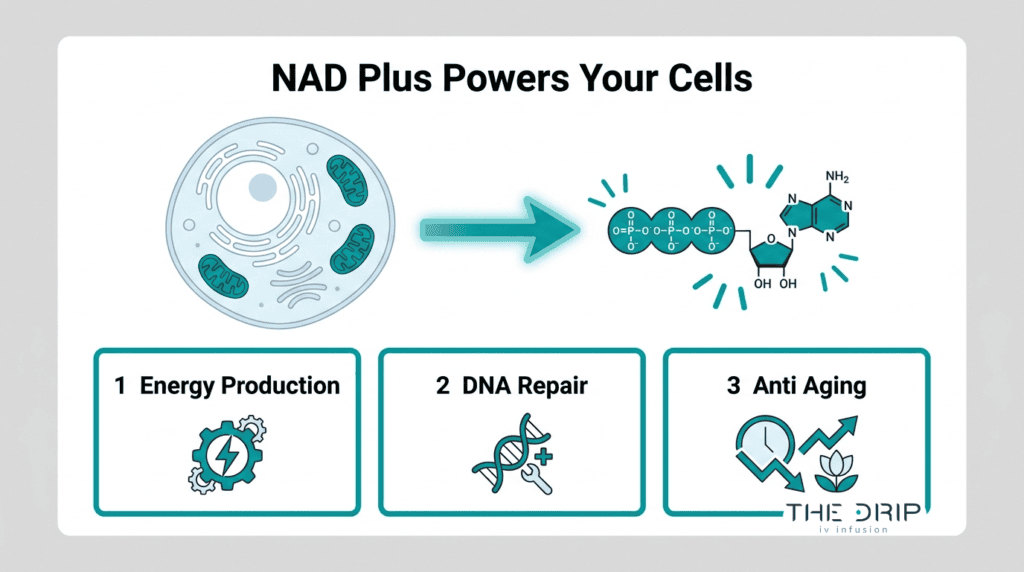
What Role Does NAD+ Play in Cellular Energy Production?
NAD+ plays a central role in cellular energy production as a critical coenzyme found in all living cells. It functions as an essential electron carrier in mitochondrial ATP production, shuttling electrons through the metabolic chain that powers every cell. Beyond energy, NAD+ serves as a necessary substrate for sirtuins and poly(ADP-ribose) polymerases (PARPs) involved in DNA repair and gene regulation.
According to Dr. David Sinclair of Harvard Medical School, “NAD+ is the closest we’ve gotten to a fountain of youth,” highlighting its role in activating sirtuins and promoting cellular longevity. Without adequate NAD+, cells cannot efficiently convert nutrients into usable energy or maintain genomic integrity. For anyone exploring ways to support cellular health, understanding this coenzyme’s dual function in both energy metabolism and protective repair mechanisms is foundational.
How Do NAD+ Levels Change as You Age?
NAD+ levels change as you age by declining progressively, with measurable reductions beginning in middle adulthood. MRI-based studies have demonstrated that NAD+ levels in the human brain decline by approximately 10% to 25% between young adulthood and old age.
This decline is partly driven by increased demand for DNA repair. A PLOS ONE study analyzing human skin samples from participants aged 15 to 77 found that PARP activity significantly increased with age in males (p<0.0001; r=0.768) and inversely correlated with tissue NAD+ levels (p=0.0003; r=-0.639). As PARP consumes more NAD+ to repair accumulating DNA damage, less remains available for energy production and sirtuin activation. While clinical trials with oral nicotinamide riboside have demonstrated 22 to 142% increases in blood NAD+ levels after two to four weeks, IV administration produces higher and more immediate plasma concentrations.
What Happens When Your NAD+ Levels Are Too Low?
When your NAD+ levels are too low, cells lose their capacity to produce sufficient ATP, repair damaged DNA, and regulate inflammatory responses. NAD+ depletion is a primary mediator of oxidative stress-induced ATP depletion, leading to metabolic dysfunction, neurodegeneration, and accelerated aging processes.
Common consequences of critically low NAD+ include:
- Chronic fatigue from impaired mitochondrial energy output.
- Cognitive decline and brain fog due to reduced neuronal metabolism.
- Accelerated visible aging as sirtuin activity drops.
- Increased inflammation from dysregulated immune signaling.
- Slower recovery from physical stress or illness.
This cascade explains why many adults over 40 report progressive energy loss and mental sluggishness. Replenishing NAD+ through targeted strategies can help interrupt this cycle before dysfunction compounds further.
Understanding how NAD+ depletion affects the body clarifies why direct replenishment methods matter.
How Does NAD+ IV Therapy Work?
NAD+ IV therapy works by delivering nicotinamide adenine dinucleotide directly into the bloodstream through a controlled intravenous infusion. The subsections below cover why IV delivery is preferred, what happens during a session, and how long treatment takes.
Why Is NAD+ Delivered Intravenously Instead of Orally?
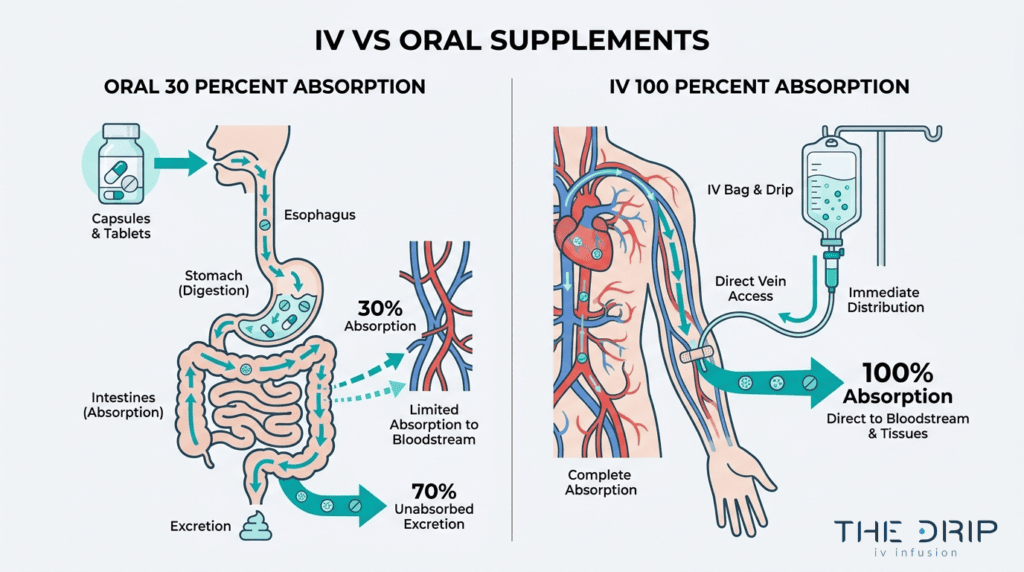
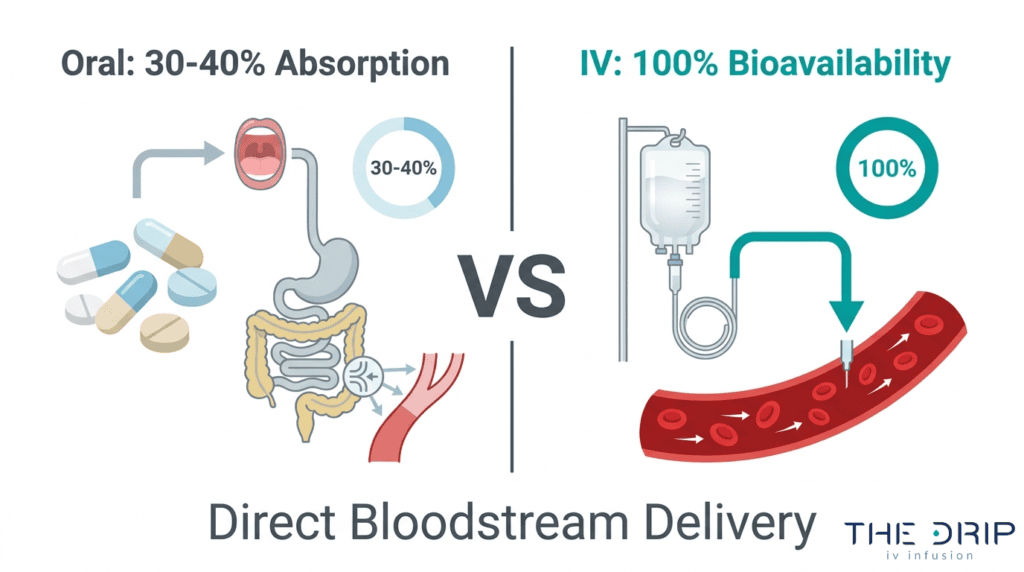
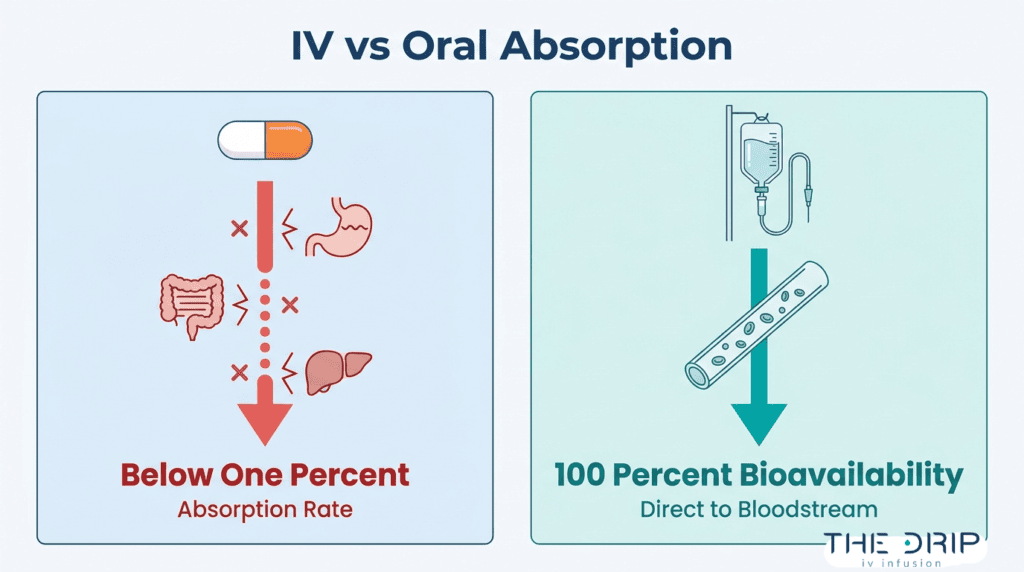
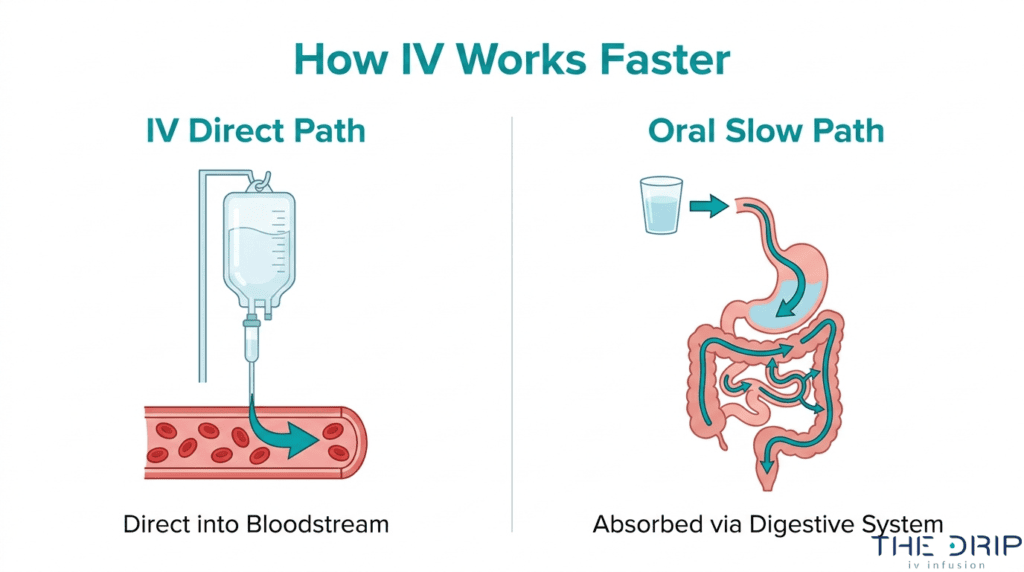
NAD+ is delivered intravenously instead of orally because IV administration achieves near 100% bioavailability by bypassing the gastrointestinal tract and hepatic first-pass metabolism. Oral NAD+ precursors must survive stomach acid, intestinal absorption, and liver processing before reaching systemic circulation, which significantly limits how much active compound enters cells. The NAD+ molecule itself is too large and unstable to survive intact through digestion. Intravenous delivery eliminates these barriers entirely, placing the full dose directly into the bloodstream for immediate cellular uptake. For anyone seeking rapid, measurable increases in NAD+ levels, IV remains the most efficient route available.

What Happens During a NAD+ IV Infusion Session?
A NAD+ IV infusion session begins with a health assessment, followed by IV catheter placement and a slow, controlled drip of NAD+ solution. The infusion rate is deliberately kept low because rapid delivery commonly triggers adverse reactions, including nausea, abdominal cramping, and chest tightness often described as a heavy weight on the sternum. According to Jinfiniti Precision Medicine, typical sessions range from 2 to 4 hours to ensure patient safety and minimize these reactions. If discomfort occurs, the infusion specialist slows the rate until symptoms resolve. Clients remain seated or reclined throughout, and vitals are monitored periodically. Current NAD+ literature still lacks long-term safety data for high-dose infusions, making practitioner oversight during each session essential.

How Long Does a Typical NAD+ IV Therapy Session Take?
A typical NAD+ IV therapy session takes approximately 2 to 4 hours depending on dosage and individual tolerance. According to a 2023 study published in PubMed, patients receiving NAD+ IV therapy had a 4-day average total infusion time of 97 ± 56.33 minutes per session. Clinical protocols commonly involve dosages between 250 mg and 1,000 mg, administered weekly or as a loading dose over several consecutive days. Pricing reflects this time commitment; sessions in the U.S. range from $250 to $1,500 each, with loading dose packages of 4-6 sessions priced between $1,500 and $6,000. The extended duration compared to standard IV drips is something most first-time clients underestimate.
Understanding how NAD+ IV therapy is administered helps clarify what benefits it can deliver.
What Are the Benefits of NAD+ IV Therapy?
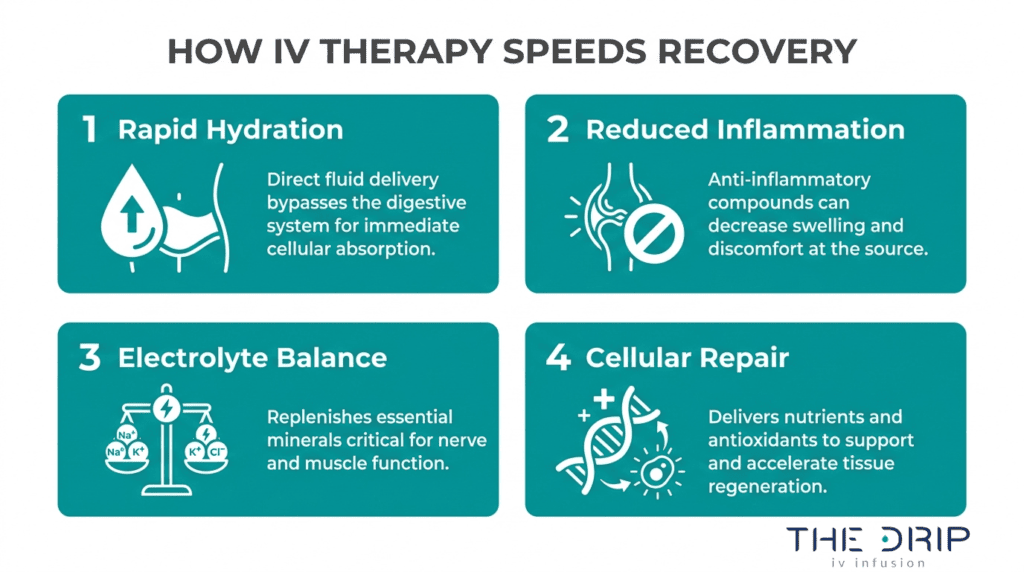
The benefits of NAD+ IV therapy span anti-aging support, cognitive enhancement, cellular energy production, DNA repair, addiction recovery, inflammation reduction, and athletic performance. Each benefit stems from restoring optimal NAD+ levels in the body.
How Does NAD+ IV Therapy Support Anti-Aging?
NAD+ IV therapy supports anti-aging by replenishing the coenzyme that activates sirtuins, the proteins responsible for cellular longevity and repair. As NAD+ levels decline with age, skin elasticity decreases, cellular turnover slows, and oxidative damage accumulates. Intravenous delivery restores these levels rapidly, supporting the body’s natural defense mechanisms against age-related deterioration. According to Dr. Fred Bloem, MD, NAD+ IV therapy promotes cellular repair and counters the biological markers of aging at the mitochondrial level. For anyone noticing the visible and internal signs of aging, this represents one of the most direct interventions available for supporting cellular youth.
How Does NAD+ IV Therapy Improve Cognitive Function?
NAD+ IV therapy improves cognitive function by restoring mitochondrial homeostasis in brain cells starved of adequate energy. When NAD+ levels drop, oxidative stress depletes ATP, triggering metabolic dysfunction and neurodegeneration. Clinical data published on ResearchGate indicates that NAD+ administration improves cognitive function and reduces neuroinflammation in models of chronic cerebral hypoperfusion by restoring mitochondrial homeostasis. This makes NAD+ IV therapy particularly relevant for individuals experiencing brain fog, mental fatigue, or early signs of cognitive decline. By reducing neuroinflammation and supporting healthy mitochondrial output, the therapy helps sharpen focus, memory, and mental clarity.
How Does NAD+ IV Therapy Boost Cellular Energy and Metabolism?
NAD+ IV therapy boosts cellular energy and metabolism by delivering the coenzyme directly into the bloodstream, where it fuels mitochondrial ATP production. Intravenous administration achieves near 100% bioavailability by bypassing the gastrointestinal tract and hepatic first-pass metabolism, which significantly limits oral precursor absorption. As we age, chronic DNA damage activates PARP enzymes that consume NAD+ for repair, depleting the supply available for energy production. IV delivery circumvents this bottleneck, flooding cells with the substrate they need for efficient metabolic function. The resulting energy boost is often noticeable within hours of infusion rather than weeks.
How Does NAD+ IV Therapy Aid in DNA Repair?
NAD+ IV therapy aids in DNA repair by supplying the essential substrate that PARP enzymes require to fix damaged DNA strands. PARP activation is the body’s primary response to DNA breaks caused by oxidative stress, UV exposure, and environmental toxins. Without sufficient NAD+, these repair mechanisms stall, allowing mutations to accumulate and accelerating cellular aging. By restoring NAD+ to optimal levels through IV delivery, the therapy ensures PARP enzymes can function efficiently. This proactive approach to genomic maintenance supports long-term cellular integrity and reduces the risk of age-related functional decline.
How Does NAD+ IV Therapy Support Addiction Recovery?
NAD+ IV therapy supports addiction recovery by reducing cravings, anxiety, and depressive symptoms associated with substance withdrawal. A study published in Bentham Open’s Current Psychopharmacology demonstrated a significant relationship between NAD+ infusions and decreasing scores for substance cravings (P=0.015) and anxiety (P=0.003) in addiction recovery populations. The therapy works by replenishing neurotransmitter precursors and restoring brain chemistry disrupted by prolonged substance use. Rather than masking withdrawal symptoms, NAD+ IV therapy addresses the underlying cellular depletion that makes early recovery so physically and mentally challenging.
How Does NAD+ IV Therapy Reduce Inflammation?
NAD+ IV therapy reduces inflammation by modulating immune responses and lowering pro-inflammatory markers throughout the body. NAD+ supplementation has been shown to reduce CRP and cytokine levels in patients with chronic inflammatory conditions, according to research published in Ageing Research Reviews. The NAD+ metabolome includes related compounds such as NADH, NADP+, NADPH, and precursors like nicotinamide mononucleotide (NMN) and nicotinamide riboside (NR), all of which participate in the body’s antioxidant defense systems. For those dealing with chronic pain, autoimmune flare-ups, or persistent low-grade inflammation, this pathway offers meaningful cellular-level relief.
How Does NAD+ IV Therapy Enhance Athletic Performance?
NAD+ IV therapy enhances athletic performance primarily through improved recovery and cellular energy restoration rather than direct performance gains during exercise. According to a systematic review published in Clinical and Translational Medicine, while NAD+ precursors can increase blood levels, there is currently no conclusive evidence that they improve athletic performance in healthy, young individuals. However, the recovery benefits remain compelling: faster ATP regeneration, reduced oxidative damage from intense training, and improved mitochondrial function all contribute to shorter recovery windows. For serious athletes, this translates to more consistent training capacity over time.
With these wide-ranging benefits established, understanding who stands to gain the most helps determine whether NAD+ IV therapy aligns with your health goals.
Who Is a Good Candidate for NAD+ IV Therapy?
Good candidates for NAD+ IV therapy include adults experiencing age-related decline, chronic fatigue, brain fog, or those seeking accelerated athletic recovery. The following profiles outline who benefits most.
Who Should Consider NAD+ IV Therapy for Age-Related Decline?
Adults experiencing age-related decline should consider NAD+ IV therapy when natural NAD+ levels have dropped significantly. Since NAD+ depletion accelerates metabolic dysfunction and neurodegeneration through oxidative stress-induced ATP loss, individuals noticing declining energy, slower recovery, or visible aging signs after age 40 are strong candidates. According to a study published in Frontiers in Endocrinology involving 1,518 participants, whole blood NAD+ contents in men significantly declined with aging, with a notable decrease observed in the 40–49 years age group compared to those under 30. This age-dependent drop makes proactive NAD+ replenishment particularly relevant for adults in midlife and beyond.
Who Should Consider NAD+ IV Therapy for Chronic Fatigue?
Individuals with chronic fatigue should consider NAD+ IV therapy when persistent exhaustion does not resolve with conventional rest or lifestyle changes. NAD+ plays an essential role in mitochondrial ATP production, and depleted levels directly compromise cellular energy output. People experiencing unrelenting tiredness, reduced stamina, or difficulty completing daily tasks despite adequate sleep often present with underlying NAD+ insufficiency. Because intravenous delivery achieves near-complete bioavailability, it offers a more direct route to restoring cellular energy than oral alternatives. For those whose fatigue has become a barrier to normal functioning, NAD+ IV therapy provides targeted metabolic support at the mitochondrial level.
Who Should Consider NAD+ IV Therapy for Brain Fog?
Individuals experiencing brain fog should consider NAD+ IV therapy when cognitive symptoms like poor concentration, mental slowness, or memory lapses persist without clear medical explanation. NAD+ supports neuronal health by fueling mitochondrial energy production in brain cells and activating sirtuins involved in neuroprotection. When NAD+ levels decline, the brain becomes vulnerable to neuroinflammation and oxidative damage that manifests as cognitive sluggishness. This therapy is especially worth considering for professionals, students, or older adults whose mental clarity directly affects quality of life or work performance.
Who Should Consider NAD+ IV Therapy for Athletic Recovery?
Athletes and active individuals should consider NAD+ IV therapy for recovery when intense training creates sustained soreness, prolonged muscle fatigue, or slower performance rebounds. NAD+ supports the cellular repair mechanisms that muscles rely on after high-intensity exertion, including DNA repair pathways and mitochondrial regeneration. While systematic reviews suggest NAD+ precursors have not conclusively improved athletic performance in healthy young individuals, the recovery and cellular restoration benefits remain relevant for those pushing physical limits consistently. For athletes prioritizing faster turnaround between sessions, NAD+ IV therapy addresses recovery at a cellular level that nutrition alone may not reach.
With candidate profiles clarified, understanding what to expect before and after treatment helps you prepare effectively.
What Should You Expect Before and After NAD+ IV Treatment?
You should expect a preparation phase, potential side effects during infusion, and gradual improvements afterward. The following sections cover pre-session preparation, common reactions during treatment, and post-therapy results.
How Should You Prepare for a NAD+ IV Therapy Session?
You should prepare for a NAD+ IV therapy session by hydrating well, eating a light meal, and allowing adequate time in your schedule. Since sessions can last 2 to 4 hours, planning accordingly reduces stress and improves comfort.
Key preparation steps include:
- Drinking 16–32 oz of water in the hours before your appointment.
- Eating a balanced snack or light meal to reduce nausea risk.
- Wearing comfortable clothing with easy access to your forearm.
- Avoiding alcohol and caffeine for at least 12 hours prior.
- Communicating any medications or health conditions to your infusion specialist.
Arriving relaxed and well-nourished helps your body tolerate the infusion more smoothly, particularly at higher dosages.
What Side Effects Might You Experience During Infusion?
The side effects you might experience during infusion include nausea, abdominal cramping, and chest tightness. These sensations are commonly reported and typically described as a heavy weight on the sternum. Most resolve quickly when the infusion rate is slowed.
According to comparative research published on medRxiv, nicotinamide riboside (NR) delivered intravenously is associated with fewer and less severe adverse experiences during infusion compared to NAD+ IV. This suggests that the NAD+ molecule itself, rather than the IV delivery method, contributes to these temporary discomforts.
For most clients, side effects remain mild and manageable. Communicating any discomfort to your infusion specialist allows real-time rate adjustments that significantly improve tolerance.
What Results Can You Expect After NAD+ IV Therapy?
The results you can expect after NAD+ IV therapy include improved mental clarity, increased energy, and reduced feelings of fatigue. Because IV delivery achieves near 100% bioavailability, many clients notice effects within 24 to 48 hours of their first session.
Common post-treatment outcomes include:
- Enhanced focus and reduced brain fog.
- Steadier energy levels throughout the day.
- Improved mood and reduced feelings of anxiety.
- Better sleep quality in the days following treatment.
Results vary based on baseline NAD+ levels, dosage, and overall health status. Loading dose protocols over several consecutive days often produce more pronounced initial improvements compared to single sessions. Ongoing maintenance treatments help sustain these benefits over time, which leads naturally into determining ideal treatment frequency.
How Often Should You Get NAD+ IV Therapy?
NAD+ IV therapy frequency depends on your specific health goal. Anti-aging, energy restoration, and long-term maintenance each require different scheduling protocols.
How Often Should You Get NAD+ IV Therapy for Anti-Aging?
You should get NAD+ IV therapy for anti-aging every one to two weeks during an initial loading phase, then transition to monthly sessions. Clinical protocols often involve dosages between 250 mg and 1,000 mg per session, typically administered weekly or as a loading dose over several consecutive days, according to Olympia Pharmacy. Most anti-aging protocols begin with four to six consecutive or closely spaced sessions to rapidly restore depleted cellular NAD+ levels, followed by monthly maintenance infusions. Since PARP activity increases with age and continuously depletes NAD+ reserves, consistent replenishment matters more than occasional high-dose treatments.
How Often Should You Get NAD+ IV Therapy for Energy?
You should get NAD+ IV therapy for energy every one to two weeks until fatigue symptoms resolve, then reduce to biweekly or monthly sessions. Energy-focused protocols typically use moderate doses of 250 mg to 500 mg, since the primary goal is sustaining mitochondrial ATP production rather than deep cellular repair. Clients experiencing chronic fatigue often benefit from an initial series of weekly infusions over three to four weeks. Once energy levels stabilize, spacing sessions further apart helps maintain results without over-scheduling. For most people seeking sustained vitality, the transition from weekly to maintenance dosing happens within the first month.
How Often Should You Get NAD+ IV Therapy for Maintenance?
You should get NAD+ IV therapy for maintenance once every two to four weeks after completing an initial loading protocol. Maintenance frequency depends on factors such as:
- Age and baseline NAD+ depletion rate
- Lifestyle stressors including sleep quality and exercise intensity
- Individual metabolic response to prior infusions
Because NAD+ levels decline progressively with age, particularly after 40, ongoing maintenance prevents the gradual return of symptoms like brain fog and low energy. For most healthy adults using NAD+ IV therapy as preventive wellness support, monthly sessions at 250 mg to 500 mg sustain elevated cellular NAD+ without requiring the intensity of therapeutic loading doses.
With frequency established, understanding costs helps you plan a sustainable treatment schedule.
How Much Does NAD+ IV Therapy Cost?
NAD+ IV therapy costs between $250 and $1,500 per single session in the U.S. market. Pricing varies based on dosage, provider type, and whether sessions are purchased individually or as loading dose packages.
Several factors influence the total investment:
- Dosage: Sessions range from 250 mg to 1,000 mg, with higher doses commanding higher prices.
- Package pricing: Loading dose packages of 4–6 sessions typically cost between $1,500 and $6,000.
- Mobile service fees: Mobile IV therapy providers often charge a base fee starting around $199, with NAD+ add-ons priced by dosage (for example, $100 for 100 mg up to $800 for 1,000 mg).
- Session duration: Longer infusion times of 2–4 hours contribute to higher service costs compared to standard vitamin drips.
According to Global Clinic, the wide price range reflects differences in clinical setting, geographic market, and whether patients receive standalone NAD+ or combination formulas with additional nutrients.
For most people seeking anti-aging or cognitive benefits, the per-session cost matters less than the cumulative investment across a full protocol. A maintenance schedule of monthly sessions represents a more sustainable long-term expense than intensive loading doses, making it worth discussing protocol options with your provider before committing.
Understanding therapy costs helps you evaluate whether NAD+ IV fits within your broader wellness plan and safety expectations.
Is NAD+ IV Therapy Safe and Backed by Science?
NAD+ IV therapy is generally safe when administered by qualified professionals, though research is still evolving. The following sections cover current scientific evidence and potential risks.
What Does the Research Say About NAD+ Supplementation?
The research on NAD+ supplementation shows promising but still developing evidence. Clinical studies have demonstrated measurable outcomes, including reduced substance cravings, decreased anxiety, and lower depression scores in addiction recovery populations. NAD+ supplementation has also been shown to modulate immune function by reducing pro-inflammatory markers such as CRP and cytokines.
However, important limitations exist. According to a systematic review published in Clinical and Translational Medicine, while NAD+ precursors can increase blood levels, there is currently no conclusive evidence that they improve athletic performance in healthy, young individuals. Long-term safety data for high-dose infusions remains insufficient, and comparative research between different IV precursors is limited.
For most wellness applications, the existing data supports biological plausibility rather than definitive clinical proof, making provider expertise and proper protocols essential.
Are There Any Risks or Contraindications for NAD+ IV Therapy?
The risks of NAD+ IV therapy include mild to moderate side effects and regulatory considerations. Common adverse reactions during infusion include:
- Nausea and abdominal cramping
- Chest tightness, often described as a heavy weight on the sternum
- Discomfort at the infusion site
These symptoms typically resolve by slowing the infusion rate. According to Browne Jacobson’s 2026 analysis of the cosmetic IV therapy market, legal risks in this largely unregulated space include potential medical malpractice liability for injuries such as extravasation.
Choosing a provider that uses pharmaceutical-grade NAD+ and employs experienced infusion specialists significantly reduces these risks. Individuals with active infections, certain cardiovascular conditions, or those who are pregnant should consult their healthcare provider before treatment.
Understanding safety considerations helps inform the next step: comparing NAD+ IV therapy to alternative supplementation methods.
How Does NAD+ IV Therapy Compare to Other NAD+ Supplements?
NAD+ IV therapy compares to other NAD+ supplements primarily through differences in bioavailability, onset speed, and delivery method. The following subsections break down how IV delivery stacks up against oral NMN, oral NR, and nasal spray options.
How Does NAD+ IV Therapy Compare to Oral NMN Supplements?
NAD+ IV therapy compares to oral NMN supplements through superior bioavailability and faster cellular delivery. IV administration bypasses the gastrointestinal tract entirely, while oral NMN must survive stomach acid and undergo hepatic first-pass metabolism before conversion to NAD+ in tissues.
Key differences include:
- NAD+ IV delivers the coenzyme directly into the bloodstream at near 100% bioavailability.
- Oral NMN requires enzymatic conversion through intermediate steps before raising intracellular NAD+ levels.
- IV sessions produce immediate plasma concentration spikes, whereas oral NMN builds levels gradually over weeks.
- NMN capsules offer daily convenience without clinical visits, though absorption rates vary significantly between individuals.
For those prioritizing rapid, measurable NAD+ elevation, IV therapy remains the most direct route. Oral NMN suits individuals seeking a lower-cost daily maintenance strategy with less immediate impact.
How Does NAD+ IV Therapy Compare to Oral NR Supplements?
NAD+ IV therapy compares to oral NR supplements by delivering higher immediate plasma concentrations with fewer required conversion steps. Nicotinamide riboside enters cells and undergoes phosphorylation to NMN before final conversion to NAD+, adding metabolic steps that reduce efficiency.
Clinical trials have demonstrated 22–142% increases in blood NAD+ levels after 2–4 weeks of oral NR supplementation, according to research published by Inner Balance, though IV administration produces higher and more immediate plasma concentrations.
Practical distinctions include:
- Oral NR requires daily dosing over multiple weeks to achieve meaningful NAD+ elevation.
- NAD+ IV provides acute, session-based boosts suited to targeted therapeutic goals.
- NR capsules cost significantly less per month than recurring IV sessions.
- IV therapy requires clinical oversight, while NR is available as an over-the-counter supplement.
Each approach serves different needs; IV therapy is better suited for acute interventions, while oral NR works as an accessible long-term maintenance tool.
How Does NAD+ IV Therapy Compare to NAD+ Nasal Sprays?
NAD+ IV therapy compares to NAD+ nasal sprays through substantially different absorption pathways and regulatory oversight. Nasal sprays attempt to deliver NAD+ through the nasal mucosa, offering convenience but with limited published bioavailability data. IV delivery, by contrast, achieves complete systemic availability immediately.
NAD+ remains on the FDA 503A Bulks List Category 1, meaning it is generally accepted for use in pharmacy compounding for individual patient prescriptions. This regulatory status supports IV formulations compounded under proper pharmacy standards, while nasal spray products often lack equivalent quality controls.
Important considerations:
- Nasal sprays have no established standardized dosing protocols backed by clinical trials.
- IV therapy operates within a compounding pharmacy framework with FDA-recognized ingredient standards.
- Absorption through nasal mucosa remains poorly quantified compared to intravenous bioavailability data.
For individuals seeking verified NAD+ delivery with regulatory backing, IV therapy offers a more substantiated option than nasal sprays, which remain largely unstudied in controlled settings.
With delivery methods clarified, mobile NAD+ IV services can further simplify access to this therapy.
How Can Mobile NAD+ IV Therapy Enhance Your Experience?
Mobile NAD+ IV therapy enhances your experience by eliminating travel to a clinic and allowing treatment in a comfortable, familiar environment. The following sections cover how The Drip IV Infusion simplifies care and the key takeaways about NAD+ IV therapy benefits.
Can The Drip IV Infusion’s Mobile NAD+ Service Simplify Care?
Yes, The Drip IV Infusion’s mobile NAD+ service simplifies care by bringing nurse-administered infusions directly to your home or workplace. Since NAD+ IV sessions can last several hours, receiving treatment in a relaxed setting makes the extended infusion time far more comfortable than sitting in a clinical environment.
The Drip IV Infusion was founded in Fall 2022 by professionals with decades of experience in nursing, emergency medicine, and IV medical techniques. This mobile-first model reflects a rapidly growing industry; according to Grand View Research, the global mobile IV hydration services market was estimated at USD 1.3 billion in 2024 and is projected to grow at a CAGR of 9.8% through 2030.
The Drip IV Infusion offers NAD+ as a specialty treatment targeting inflammation reduction, mental restoration, anti-aging, and addiction recovery support. For those managing demanding schedules or chronic fatigue, the convenience of at-home delivery removes the single biggest barrier to consistent treatment.
What Are the Key Takeaways About NAD+ IV Therapy Benefits?
The key takeaways about NAD+ IV therapy benefits center on cellular restoration, cognitive support, and long-term wellness optimization. The most actionable insights from this article include:
- NAD+ is essential for mitochondrial energy production, DNA repair, and sirtuin activation, and its levels decline significantly with age.
- Intravenous delivery achieves near 100% bioavailability, making it the most direct method for replenishing cellular NAD+ stores.
- Clinical evidence supports benefits for cognitive function, inflammation reduction, and addiction recovery.
- Sessions typically last 2 to 4 hours with dosages between 250 mg and 1,000 mg, so planning for extended infusion time is important.
- Mobile NAD+ IV therapy eliminates clinic visits, which is especially practical given the longer session durations.
- Ideal candidates include adults experiencing chronic fatigue, brain fog, age-related decline, or those seeking enhanced recovery.
For most people exploring NAD+ IV therapy, consistency matters more than any single session. A mobile service that fits into your routine makes sustained treatment protocols realistic rather than aspirational. The Drip IV Infusion brings this accessibility to Arizona with experienced nurses, customizable add-ons, and a focus on personalized wellness partnerships.