IV insertion is the process of placing a peripheral intravenous catheter into a vein to deliver fluids, medications, or nutrients directly into the bloodstream. Successful cannulation depends on preparation, vein selection, precise technique, and ongoing site management.
This guide covers pre-insertion preparation, vein selection and difficult-access strategies, step-by-step catheter insertion technique, first-stick success optimization, special patient populations, common mistakes and complication management, pain reduction and infection prevention, and long-term skill development.
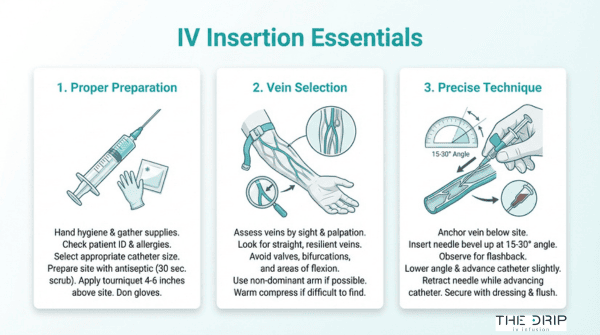
Preparation begins with gathering the right supplies, matching catheter gauge to therapy type, assessing the patient’s medical history, and verifying the physician’s order. Selecting the correct gauge alone prevents one of the most common causes of insertion-related phlebitis.
Vein selection requires both visual and tactile assessment across hand, forearm, and antecubital sites while avoiding areas of flexion, prior damage, or valve obstruction. When standard methods fail, layered strategies like tourniquet adjustment, warm compresses, gravity positioning, and ultrasound guidance help locate deeper or non-palpable vessels.
The insertion sequence itself follows a strict order: tourniquet application, site disinfection, vein anchoring, controlled needle entry at 10 to 30 degrees, flashback confirmation, catheter advancement, securement, and saline flush verification. Each step builds on the previous one, and skipping any of them introduces avoidable risk.
Adapting technique for pediatric, elderly, obese, dehydrated, dark-skinned, and pregnant patients requires shifting from visual-first to palpation-first strategies and adjusting catheter size, angle, and positioning for each group’s anatomy.
Recognizing complications like infiltration, phlebitis, and extravasation early, combined with proper securement and aseptic maintenance, protects patients after the catheter is placed. Simulation training and first-stick tracking then close the loop between knowledge and consistent clinical performance.
Why Is Proper IV Insertion Technique So Important?
Proper IV insertion technique is important because it directly prevents mechanical complications that can harm patients. According to StatPearls (NCBI), proper IV site selection and insertion technique are critical to preventing mechanical complications such as air embolism and thrombosis. Even a small procedural error, whether in angle, depth, or site choice, can trigger complications that escalate quickly from minor discomfort to serious vascular events. For clinicians and mobile IV therapy professionals alike, mastering correct technique is not optional; it is the foundation that every other tip and strategy in this guide builds upon. The sections that follow cover preparation, vein selection, step-by-step insertion methods, and complication management to help sharpen that foundation.
How Should You Prepare Before Starting an IV Insertion?
You should prepare before starting an IV insertion by gathering supplies, selecting the correct catheter gauge, assessing the patient, and verifying the physician’s order. Each step below covers one essential preparation task.
What Supplies and Equipment Do You Need for IV Insertion?
The supplies and equipment you need for IV insertion include:
- Appropriately sized IV catheter (gauge selected based on therapy type)
- Tourniquet
- Antiseptic solution (chlorhexidine or alcohol swabs)
- Sterile transparent dressing or tape
- Pre-filled normal saline flush syringe
- Extension set or T-connector
- Clean gloves (non-sterile for peripheral access)
- Sharps disposal container
- Labels and documentation materials
Having everything within arm’s reach before gloving prevents interruptions that compromise aseptic technique. This single habit separates consistently clean insertions from avoidable contamination events.
How Do You Select the Right IV Catheter Gauge?
You select the right IV catheter gauge by matching catheter size to the prescribed therapy and the patient’s vein condition. According to the Merck Manuals, 18- or 20-gauge IV catheters are typically used for routine infusions in adults, while 14- or 16-gauge catheters are selected for high-volume infusions such as rapid fluid resuscitation or blood transfusions.
Smaller gauges, like 22 or 24, suit pediatric patients and adults with small, fragile veins. Choosing the smallest gauge that delivers the required flow rate protects vein integrity and reduces phlebitis risk. Oversizing the catheter relative to the vein is one of the most preventable causes of insertion-related complications.
What Patient Assessment Should You Complete Before IV Insertion?
The patient assessment you should complete before IV insertion covers medical history, allergy status, coagulation risk, and skin integrity at potential insertion sites. Review the patient’s current medications, particularly anticoagulants, which increase bleeding risk during cannulation.
Inspect both arms for bruising, scarring, infection, or prior infiltration. Patients with mastectomy history, arteriovenous fistulas, or lymphedema on one side require access on the opposite extremity. The CDC recommends chlorhexidine-impregnated dressings for patients aged 18 years and older to protect short-term central venous catheter sites, highlighting how site protection decisions begin during this assessment phase.
How Should You Verify the Order and Confirm Patient Identity?
You should verify the order and confirm patient identity by performing a two-patient-identifier check before any IV insertion. Match the patient’s name and date of birth against the physician’s order, the medication administration record, and the patient’s wristband.
Confirm the prescribed solution, infusion rate, and route. This verification step catches transcription errors and wrong-patient scenarios before a needle ever touches skin. Skipping this step remains one of the most common sources of IV administration errors. With identity and order confirmed, the next priority is selecting the best available vein.
How Do You Choose the Best Vein for IV Insertion?
You choose the best vein for IV insertion by assessing visibility, palpability, and location while avoiding sites prone to complications. Common failures such as off-shot insertion, shallow puncture, and double puncture of the vein wall often trace back to poor vein selection.
What Makes a Vein Ideal for Peripheral IV Access?
A vein ideal for peripheral IV access is one that feels bouncy and resilient on palpation, appears straight for an adequate length, and sits in a location away from joints or areas of flexion. Ideal veins refill quickly after compression and are large enough to accommodate the selected catheter gauge.
Keeping the arm in a dependent position maximizes pooling of venous blood, making suitable veins easier to identify. According to standards introduced by the Australian Commission on Safety and Quality in Health Care, proper vein assessment and catheter management reduce complications and improve vascular access outcomes. A vein that looks prominent but feels hard or cord-like often indicates sclerosis, making it a poor candidate despite its visual appeal.
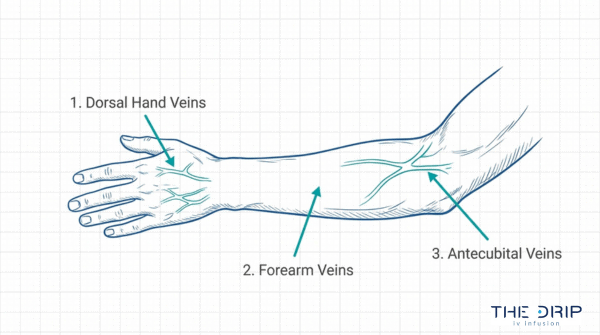
Which Veins in the Hand Are Best for IV Insertion?
The veins in the hand best for IV insertion are the dorsal metacarpal veins and the dorsal venous network. These superficial vessels sit on the back of the hand, where they are typically visible and easy to palpate.
Dorsal metacarpal veins run between the knuckles and offer short, straight segments suitable for smaller-gauge catheters. The dorsal venous arch connects these tributaries and provides a slightly larger target. Hand veins work well for short-duration infusions, though they can be more painful due to thinner overlying tissue. Starting distally preserves proximal sites for future access if needed.
Which Veins in the Forearm Are Best for IV Insertion?
The veins in the forearm best for IV insertion are the cephalic vein and the accessory cephalic vein. Both run along the lateral (thumb-side) aspect of the forearm and provide long, straight segments with adequate caliber.
- The cephalic vein travels from the wrist toward the elbow along the radial side, offering consistent depth and stability.
- The accessory cephalic vein branches off the cephalic vein and provides an alternative when the primary vessel is unavailable.
- The basilic vein on the medial forearm is another option, though its proximity to nerves and deeper position require more cautious palpation.
Forearm sites are generally preferred for most infusions because the area allows secure catheter stabilization and comfortable patient movement.
Which Veins in the Antecubital Fossa Are Best for IV Insertion?
The veins in the antecubital fossa best for IV insertion are the median cubital vein, the cephalic vein, and the basilic vein where they converge at the inner elbow. The median cubital vein is the most commonly targeted because it is large, superficial, and well-anchored by surrounding tissue.
These veins accommodate larger-gauge catheters and support rapid fluid delivery or blood draws. However, antecubital sites sit at a point of flexion, which increases the risk of catheter kinking and dislodgement during patient movement. For this reason, experienced clinicians typically reserve antecubital veins for short-term access, blood sampling, or emergency situations rather than extended infusions.
What Veins Should You Avoid During IV Insertion?
The veins you should avoid during IV insertion include those in areas of flexion, near previous puncture sites, and over joints. Clinicians should also avoid veins in an extremity affected by injury, surgery, or lymphedema.
Specific veins and sites to avoid include:
- Veins of the lower extremities, which carry a higher risk of thrombophlebitis.
- The inner wrist, where nerves and tendons sit dangerously close to the vein.
- Previously infiltrated or phlebitic sites that may be damaged.
- Veins that feel hard, tortuous, or sclerosed on palpation.
- Areas near arteriovenous fistulas used for dialysis.
According to Pressbooks Nursing Advanced Skills guidelines, clinicians should avoid areas of flexion and must secure all catheters with a stabilization device to prevent accidental dislodgement. Selecting the right vein from the start sets the foundation for the techniques used to locate and access it.
What Techniques Help You Find Difficult Veins?
Techniques that help you find difficult veins range from simple physical methods to advanced imaging technology. The following sub-sections cover tourniquets, gravity positioning, warm compresses, tactile stimulation, vein finders, and ultrasound guidance.
How Does Applying a Tourniquet Improve Vein Visibility?
Applying a tourniquet improves vein visibility by restricting venous return, which causes blood to pool in the veins below the constriction point. This pooling engorges the vessels, making them more palpable and easier to see beneath the skin. Place the tourniquet 3 to 4 inches above the intended insertion site, tight enough to impede venous flow without occluding arterial supply. The patient should still have a palpable radial pulse. If veins remain flat after application, ask the patient to open and close their fist several times to promote additional engorgement.
How Does Gravity Help Engorge Veins Before IV Insertion?
Gravity helps engorge veins before IV insertion by encouraging venous blood to pool in the dependent extremity. Lowering the patient’s arm below heart level allows blood to fill peripheral veins more fully, increasing vessel diameter and improving palpability. This technique works especially well when combined with tourniquet application. For patients with chronically difficult access, having them dangle the arm over the side of the bed for 30 to 60 seconds before assessment can make a meaningful difference. In my experience, gravity is one of the most underused strategies; it costs nothing and consistently improves vein presentation when other methods fall short.
Can Warm Compresses Help Dilate Hard-to-Find Veins?
Yes, warm compresses can help dilate hard-to-find veins. Heat causes vasodilation, increasing blood flow to the area and expanding vein diameter. Apply a warm, moist towel or commercial heat pack to the target site for two to four minutes before attempting access. This approach is particularly effective for patients whose veins constrict due to cold environments, anxiety, or dehydration. Avoid excessive heat that could burn fragile skin, especially in elderly or neuropathic patients. Combining warmth with a tourniquet and gravity creates a layered strategy that maximizes vein presentation before the first stick.
How Does Tapping or Stroking the Vein Aid Visualization?
Tapping or stroking the vein aids visualization by triggering local vasodilation through mechanical stimulation. Gentle, rapid taps over the target vessel release histamine from surrounding tissue, which relaxes the vein wall and promotes engorgement. This makes the vein more prominent under the skin. Use light, controlled flicking rather than forceful slapping, which can cause the vein to spasm and retract. Stroking the vein distally to proximally while the tourniquet is applied can also push pooled blood into the target segment. This low-tech method pairs well with warm compresses for patients who have small or deeply seated veins.
When Should You Use a Vein Finder or Transilluminator?
You should use a vein finder or transilluminator when standard visual and tactile assessment fails to identify a suitable vessel. Near-infrared (NIR) vein finders project a map of subcutaneous veins onto the skin surface, revealing vessels invisible to the naked eye. These devices are especially valuable for pediatric patients, individuals with dark skin tones, and those with obesity or chronic IV access history. According to a ScienceDirect review, NIR light devices reduce peripheral IV cannulation time by 29.43 seconds and decrease attempts by 0.47 compared to traditional methods. For any clinician who routinely encounters difficult access, a vein finder is a worthwhile investment.
How Can Ultrasound-Guided IV Insertion Help with Difficult Access?
Ultrasound-guided IV insertion helps with difficult access by providing real-time visualization of deep or non-palpable veins beneath the skin surface. The clinician uses a linear probe to identify the vessel, confirm its patency, and guide the needle directly into the lumen under live imaging. A 2025 trial published in the National Institutes of Health reported a first-attempt success rate of 85.7% for ultrasound-guided peripheral IV catheter insertion. Guidewire-assisted PIVCs are also emerging in emergency departments to further improve success in patients with difficult venous access. Despite its effectiveness, confidence in this technique varies widely; only 26.1% of general staff nurses report confidence compared to 85.4% of specialized vascular access nurses. Dedicated training closes this gap and makes ultrasound guidance a reliable option across clinical settings.
With difficult veins located, the next step is mastering the insertion technique itself.
What Are the Step-by-Step Techniques for IV Catheter Insertion?
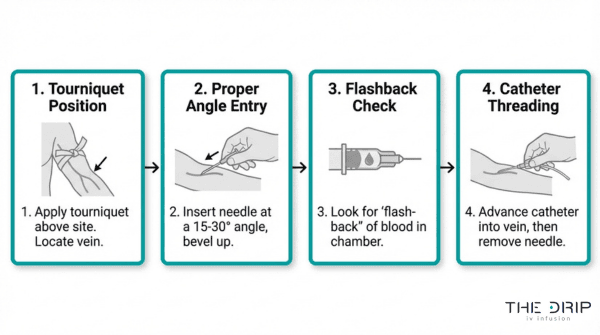
The step-by-step techniques for IV catheter insertion follow a consistent sequence: tourniquet application, site disinfection, vein anchoring, needle insertion, flashback confirmation, catheter advancement, securement, and flush verification.
How Do You Properly Apply the Tourniquet?
You properly apply the tourniquet by placing it 3 to 4 inches above the intended insertion site and tightening it enough to occlude venous flow without cutting off arterial circulation. The patient should still have a palpable radial pulse below the tourniquet. Tie it using a quick-release knot so removal is immediate once venous access is established. According to a 2023 study published by the National Institutes of Health, tourniquet use for less than 2 hours is proven safe, while longer durations increase the risk of nerve injury or tissue ischemia. For most routine IV starts, the tourniquet should remain in place no longer than one to two minutes before reassessing.
What Is the Correct Way to Disinfect the Insertion Site?
The correct way to disinfect the insertion site is to apply a chlorhexidine-based antiseptic in a back-and-forth friction scrub for at least 30 seconds, then allow the area to air dry completely. Isopropyl alcohol (70%) serves as an acceptable alternative when chlorhexidine is unavailable. Never blow on, fan, or touch the prepped area after disinfection. Allowing full drying time is essential because inserting through a wet antiseptic layer can introduce chemicals into the vein and compromise the bactericidal effect. This single preparatory step remains one of the most effective measures against catheter-related bloodstream infections.
How Do You Anchor the Vein Before Needle Entry?
You anchor the vein before needle entry by placing your non-dominant thumb approximately 1 to 2 inches below the intended puncture site and applying gentle downward traction to stretch the skin taut. This stabilization prevents the vein from rolling laterally during needle advancement. For particularly mobile veins, applying counter-traction with a second finger above the site creates a more stable target. Anchoring is especially critical in elderly patients whose veins tend to shift under loose skin. Maintaining consistent traction throughout the entire insertion, not just at the moment of puncture, significantly reduces the likelihood of a missed attempt.
What Is the Ideal Needle Insertion Angle?
The ideal needle insertion angle is 10 to 30 degrees relative to the skin surface, with the bevel facing up. Shallower angles, closer to 10 to 15 degrees, work best for superficial veins in the hand or dorsal forearm. Slightly steeper angles, approaching 25 to 30 degrees, are more appropriate for deeper veins or patients with more subcutaneous tissue. Inserting at too steep an angle risks puncturing through the posterior wall of the vein. Once you see flashback in the chamber, reduce the angle slightly before advancing to keep the catheter tip aligned within the vessel lumen.
How Do You Confirm You Have Achieved a Flashback?
You confirm you have achieved a flashback by observing a small return of blood in the catheter’s flash chamber immediately after the needle tip enters the vein lumen. This blood return appears as a visible stream or pooling of dark venous blood in the transparent hub. A true flashback indicates successful venipuncture. If no flashback appears, the needle may be positioned outside the vein or against a valve. Avoid advancing blindly without confirmation. Once flashback is visible, pause briefly, lower the insertion angle, and prepare to advance the catheter forward off the needle stylet.
How Do You Advance the Catheter and Retract the Needle?
You advance the catheter and retract the needle by first lowering the insertion angle after flashback, then sliding the catheter hub forward over the needle and into the vein using a smooth, steady motion. Never push the needle deeper to advance the catheter. Once the catheter is fully seated, apply gentle pressure over the vein just above the catheter tip to minimize blood loss, then retract and safely dispose of the needle stylet into a sharps container. Two-thirds of the catheter length should sit inside the vein to ensure stability and reduce dislodgement risk.
How Do You Secure the Catheter After Successful Insertion?
You secure the catheter after successful insertion by applying a transparent, semi-permeable dressing over the insertion site and using a manufactured stabilization device to anchor the catheter hub. Proper securement prevents migration, accidental dislodgement, and phlebitis. First-attempt success in pediatric patients ranges from only 33% to 50%, according to Wiley Online Library, making reliable securement even more critical when access is hard-won. Label the dressing with the insertion date, catheter gauge, and clinician initials. Avoid excessive taping that could obscure the site, since ongoing visual assessment of the insertion point is necessary to detect early signs of complications.
How Do You Flush and Confirm IV Patency?
You flush and confirm IV patency by connecting a prefilled normal saline syringe to the catheter hub and slowly injecting 3 to 5 mL while observing for resistance, swelling, or patient discomfort. Smooth, unimpeded flow without visible tissue swelling confirms that the catheter rests properly within the vein lumen. If resistance is felt or the patient reports burning, the catheter may be kinked, against a valve, or extravascular. Use a pulsatile (push-pause) flushing technique to create turbulence that clears the catheter interior and reduces clot formation risk. With patency confirmed, the line is ready for IV fluid or medication administration.
What Tips Improve First-Stick Success Rates?
First-stick success rates improve through proper lighting, tactile vein assessment, strategic patient positioning, careful site selection, skin stabilization, and clinician mental preparation. Each technique below addresses a specific factor.
How Does Proper Lighting Affect IV Insertion Success?
Proper lighting affects IV insertion success by allowing clinicians to visualize superficial veins, skin contours, and subtle color changes that indicate vein location. Dim or overhead-only lighting casts shadows across the arm, obscuring vein paths and increasing the likelihood of missed attempts. Positioning a direct, adjustable light source at an angle across the skin highlights vein shadows and surface topology. When visibility remains limited despite good lighting, technology-assisted approaches dramatically outperform visual inspection alone. A randomized clinical trial published on ResearchGate found that ultrasound-guided PIVC insertion achieved a 90.2% first-attempt success rate compared to 35.7% with conventional technique. Combining strong ambient light with visualization tools gives clinicians the best chance at a clean first stick.
Why Should You Palpate Rather Than Only Look for Veins?
You should palpate rather than only look for veins because tactile assessment reveals vein characteristics that visual inspection alone cannot detect. Palpation identifies vein depth, resilience, and direction beneath the skin surface. A healthy, cannulatable vein feels bouncy and springs back when pressed, while a thrombosed or sclerosed vein feels hard and cordlike. In patients with darker skin tones, deeper subcutaneous tissue, or edema, veins may be entirely invisible yet easily palpable. Running the index finger along the forearm with the tourniquet applied helps map the vein’s path and locate the straightest segment. Clinicians who rely solely on visible veins miss viable access sites, particularly in difficult-access populations where palpation becomes the primary assessment tool.
How Does Patient Positioning Impact Vein Accessibility?
Patient positioning impacts vein accessibility by using gravity to pool venous blood in the extremities. Lowering the arm below heart level engorges peripheral veins, making them more prominent and easier to palpate. Asking the patient to open and close their fist several times further increases venous distension. For patients with morbid obesity, positioning becomes even more critical; according to a 2024 study published by Termedia, ensuring that two-thirds of the catheter sits inside the vein is a significant clinical challenge due to increased subcutaneous tissue depth. Elevating the patient’s wrist slightly on a rolled towel can straighten the forearm veins and improve both visibility and angle of approach. Proper positioning is one of the simplest yet most overlooked techniques for improving first-attempt outcomes.
Why Should You Avoid Inserting Near Valves or Bifurcations?
You should avoid inserting near valves or bifurcations because these anatomical features increase the risk of catheter obstruction, vessel damage, and failed advancement. Venous valves create small, firm lumps within the vein that block catheter threading, while bifurcation points introduce irregular vessel geometry that makes smooth cannulation difficult. According to NYSORA, clinicians should target areas just above a venous bifurcation where the vessel is straighter and more stable. Valves can be identified during palpation as small, resistant bumps along the vein’s path. Selecting a straight, valve-free segment reduces the chance of catheter kinking and improves overall insertion success.
How Does Stabilizing the Skin Reduce Rolling Veins?
Stabilizing the skin reduces rolling veins by anchoring the vessel in place during needle entry. Veins embedded in loose subcutaneous tissue tend to shift laterally when the needle makes contact, causing missed punctures. Applying firm downward traction with the non-dominant thumb, approximately two to three centimeters below the intended insertion site, stretches the skin taut and locks the vein into position. This counter-tension prevents the vein from deflecting away from the needle bevel. For patients with particularly mobile veins, applying traction from both sides using the thumb and forefinger creates a stable channel. Consistent skin stabilization is one of the most reliable ways to prevent rolling, especially in elderly patients or those with lax skin.
What Mental Preparation Techniques Help Calm Nervous Clinicians?
Mental preparation techniques that help calm nervous clinicians include controlled breathing, visualization, and pre-procedure routines. Taking three slow, deep breaths before gloving activates the parasympathetic nervous system and steadies hand tremor. Visualizing the complete insertion sequence, from tourniquet application through flashback confirmation, builds procedural confidence before touching the patient. Developing a consistent setup ritual, such as arranging supplies in the same order every time, reduces cognitive load and creates a sense of control. Acknowledging nervousness rather than suppressing it also helps; experienced clinicians recognize that mild anxiety sharpens focus. For newer practitioners, these techniques bridge the gap between classroom knowledge and clinical performance, translating into more confident, successful first sticks.
How Do You Handle Special Patient Populations During IV Insertion?
You handle special patient populations during IV insertion by adapting technique, equipment, and assessment strategies to each group’s unique anatomical and physiological challenges. The sub-sections below cover pediatric, elderly, obese, dehydrated, dark-skinned, and pregnant patients.
How Do You Insert an IV in Pediatric Patients?
You insert an IV in pediatric patients by using smaller-gauge catheters, age-appropriate distraction, and topical anesthetics to reduce pain and improve cooperation. First-attempt success in this population ranges from only 33% to 50%, making preparation critical.
Applying topical numbing cream before venipuncture is standard practice, though product selection matters. A ScienceDirect study found that EMLA (lidocaine-prilocaine) cream produced significantly greater vasoconstriction at -26.28% versus -3.27% and skin blanching in 72.73% versus 25% of cases compared to 4% lidocaine. This vasoconstriction can make vein identification harder, so clinicians should map the target vein before the cream takes full effect. Securing a cooperative caregiver at bedside and using child life specialists, when available, meaningfully reduces insertion attempts.
What Techniques Work Best for Elderly Patients with Fragile Veins?
The techniques that work best for elderly patients with fragile veins include using the smallest effective catheter gauge, minimizing tourniquet pressure, and avoiding excessive skin traction. Aging reduces subcutaneous tissue and vein elasticity, making vessels prone to rolling and rupturing during cannulation.
According to a 2024 study published in the National Institutes of Health (PMC), PIVC failure occurs in 5.9% of patients overall, with phlebitis accounting for 5.8% of complications. Elderly patients face disproportionately higher rates due to vessel fragility. To reduce risk:
- Apply the tourniquet gently, just enough to distend the vein without collapsing fragile walls.
- Insert at a shallow angle, typically 10 to 15 degrees.
- Use a floating technique, advancing the catheter with a slow saline flush rather than mechanical force.
- Consider ultrasound guidance when veins are not palpable.
Patience during site selection often matters more than technique refinements in this population.
How Do You Approach IV Insertion in Obese Patients?
You approach IV insertion in obese patients by relying heavily on palpation over visualization, selecting longer catheters, and using ultrasound when surface landmarks are obscured. Increased subcutaneous tissue depth makes traditional visual assessment unreliable.
Ensuring that two-thirds of the catheter sits inside the vein is a well-established stability benchmark, yet achieving this in patients with morbid obesity presents a significant clinical challenge due to deeper tissue layers. Key strategies include:
- Prioritize the forearm over the hand, where tissue depth is often more manageable.
- Use a blood pressure cuff as a tourniquet for more even venous distension across a larger arm circumference.
- Extend the arm on a flat surface with the wrist slightly hyperextended to bring veins closer to the surface.
Ultrasound-guided insertion is particularly valuable here, as it reveals vessel depth and trajectory that neither sight nor touch can reliably detect.
What Should You Consider for IV Insertion in Dehydrated Patients?
You should consider that dehydrated patients present with flattened, poorly distended veins that resist standard cannulation techniques. Reduced circulating volume causes veins to collapse more easily under tourniquet pressure.
Pre-insertion interventions can significantly improve success:
- Apply warm compresses for two to three minutes to promote vasodilation.
- Lower the arm below heart level to encourage gravitational venous pooling.
- Use a tourniquet higher on the arm, allowing more time for slow venous filling before attempting access.
- Encourage oral fluid intake when clinically appropriate, even small amounts, before the attempt.
If peripheral access remains elusive after two attempts, escalating to ultrasound guidance or consulting a vascular access specialist prevents unnecessary patient trauma. For clinicians working in mobile or home settings, recognizing dehydration severity early guides whether peripheral access is realistic or a different approach is warranted.
How Do You Manage IV Insertion for Patients with Dark Skin Tones?
You manage IV insertion for patients with dark skin tones by shifting from visual-first to palpation-first assessment strategies. Veins that would be visible on lighter skin may not produce visible surface landmarks on darker pigmentation.
According to NURSING.com Academy, clinicians should prioritize palpation to identify suitable veins and may use alcohol swabs to enhance visualization by creating a temporary reflective surface on the skin. Additional effective techniques include:
- Palpate systematically from distal to proximal sites, feeling for the characteristic spongy bounce of a viable vein.
- Apply an alcohol swab and observe how light reflects off the moist surface to reveal subtle vein shadows.
- Use transillumination or near-infrared vein finders when palpation alone is inconclusive.
This population is often underserved by visual-only assessment protocols, making palpation skill development essential for equitable care.
What Are the Best Practices for IV Insertion in Pregnant Patients?
The best practices for IV insertion in pregnant patients include selecting the non-dominant hand or forearm, avoiding the antecubital fossa when possible to preserve mobility, and using the smallest gauge that meets therapeutic requirements. Pregnancy increases blood volume by approximately 30% to 50%, which can make veins more prominent yet also more prone to shifting due to tissue edema.
Key considerations specific to this population:
- Position the patient in a left lateral tilt or seated upright to reduce vena cava compression and improve venous return to the extremities.
- Avoid repeated tourniquet application, as pregnancy-related edema increases bruising risk.
- Communicate clearly about each step, since anxiety levels are often elevated during pregnancy.
- Secure the catheter thoroughly, as increased activity and position changes raise dislodgement risk.
With the right adaptations, population-specific IV insertion becomes a reliable, lower-stress experience for both clinician and patient.
What Are Common IV Insertion Mistakes and How Do You Avoid Them?
Common IV insertion mistakes include inserting too fast, using the wrong angle, skipping the flush, poor securement, and reinserting a retracted needle. The following subsections break down each error and how to prevent it.
Why Does Inserting Too Fast Cause Through-and-Through Punctures?
Inserting too fast causes through-and-through punctures because the needle passes completely through both walls of the vein before the clinician can react to the flashback. When speed overrides control, the bevel enters the anterior wall, blood appears in the flash chamber, but momentum carries the tip straight through the posterior wall. This results in a blown vein, hematoma formation, and a failed attempt. Slowing the advance after skin entry gives the clinician time to recognize flashback and flatten the angle before threading the catheter. A controlled, deliberate insertion pace is one of the simplest corrections that dramatically improves first-stick outcomes.
How Does Incorrect Angle Lead to Failed IV Attempts?
Incorrect angle leads to failed IV attempts because too steep an entry overshoots the vein lumen, while too shallow an approach causes the needle to ride along the vessel surface without penetrating it. According to a ResearchGate analysis of IV insertion failures, the most common causes include off-shot insertion, shallow puncture, and double puncture of the vein wall. A 15 to 30 degree insertion angle works best for most superficial peripheral veins. After flashback confirms entry, reducing the angle to nearly parallel with the skin allows smooth catheter advancement without piercing the posterior wall.
Why Is Skipping the Flush a Dangerous Shortcut?
Skipping the flush is a dangerous shortcut because it eliminates the only reliable way to confirm catheter patency and correct intravascular placement before infusing fluids or medications. Without a saline flush, an infiltrated or partially occluded catheter may go undetected until the patient develops swelling, pain, or tissue damage from extravasated solution. Flushing also clears residual blood from the catheter hub, reducing clot formation risk. This step takes seconds yet prevents complications that can require site removal, reinsertion, and extended patient discomfort. For any clinician tempted to skip this step during high-volume shifts, the time saved never justifies the downstream consequences.
How Does Poor Securement Lead to Catheter Dislodgement?
Poor securement leads to catheter dislodgement because an unstabilized catheter shifts with patient movement, gradually migrating out of the vein. It is recommended that two-thirds of the IV catheter length remain inside the vein to ensure stability and reduce dislodgement risk, according to Termedia (Maciej et al., 2024). When less than this length stays intravascular, even minor arm motion can pull the tip free. The CDC recognizes catheter stabilization as an intervention that decreases risk for phlebitis, catheter migration, and dislodgement. Using a manufactured stabilization device rather than tape alone provides consistent, secure fixation.
Why Should You Never Reinsert a Retracted Needle into the Catheter?
You should never reinsert a retracted needle into the catheter because doing so risks shearing the catheter tip, creating a plastic fragment that can embolize through the venous system. Once the needle retracts past the catheter tip, the sharp bevel faces the thin catheter wall. Pushing forward can slice through the plastic, releasing a fragment into the bloodstream that may travel to the lungs or heart. This complication, known as catheter embolism, requires interventional retrieval and poses life-threatening risk. If a catheter fails to advance properly, the correct response is to remove the entire assembly and start fresh at a new site.
Recognizing these common insertion errors is the first step; reducing patient pain and anxiety during the procedure further improves outcomes.
How Do You Minimize Patient Pain and Anxiety During IV Insertion?
You minimize patient pain and anxiety during IV insertion by combining topical anesthetics, distraction methods, clear communication, and controlled insertion speed. Each strategy targets a different dimension of the patient experience.
Does Numbing Spray or Topical Anesthetic Reduce IV Pain?
Numbing spray and topical anesthetics do reduce IV pain. Agents like lidocaine and benzocaine create localized nerve blockade at the puncture site, dulling sharp sensation before the needle penetrates the skin. According to a study published by the National Institutes of Health (PMC), topical anesthetics like lidocaine 10% and benzocaine 20% are effective in reducing pain associated with peripheral intravenous cannulation. These products work best when applied several minutes before insertion, giving the active ingredient time to absorb fully. For clinicians performing high-volume IV starts, building topical anesthetic use into the standard workflow is one of the simplest upgrades available for patient satisfaction.
How Does Distraction Technique Help Patients During IV Insertion?
Distraction technique helps patients during IV insertion by redirecting cognitive attention away from the needle and puncture sensation. Common approaches include:
- Asking the patient to take slow, deep breaths on a counted cadence.
- Engaging the patient in conversation about an unrelated topic.
- Using guided imagery or asking the patient to focus on a fixed point in the room.
- Offering a cold stimulus, such as an ice pack, on the opposite arm to shift sensory focus.
Distraction is especially effective for patients with needle phobia, because anxiety amplifies pain perception. Even brief cognitive redirection during the 5- to 10-second insertion window can meaningfully lower reported discomfort.
What Communication Strategies Ease Patient Anxiety Before the Stick?
Communication strategies that ease patient anxiety before the stick include setting expectations, using calm language, and giving the patient a sense of control. Effective techniques include:
- Explaining each step before performing it so nothing feels sudden.
- Using neutral phrasing like “pressure” or “pinch” instead of “pain” or “sting.”
- Asking the patient which arm they prefer, which fosters a feeling of autonomy.
- Maintaining a confident, unhurried tone throughout the interaction.
Patients who understand what will happen next report lower anxiety scores. In my experience, the 30 seconds spent narrating the procedure saves time on re-sticks caused by a tense, vasoconstrictive patient.
How Does Insertion Speed Affect Patient Comfort?
Insertion speed affects patient comfort by determining how much tissue resistance and drag the patient feels. A smooth, moderately paced insertion reduces pain compared to both extremes. Inserting too slowly prolongs skin contact with the needle bevel, increasing discomfort. Inserting too fast risks through-and-through puncture, which causes a sharp pain spike and often requires a second attempt. The ideal approach is a confident, steady advancement at a consistent angle once the bevel breaks the skin. Controlled speed also gives the clinician time to watch for flashback without overshooting the vein.
With pain and anxiety managed effectively, maintaining sterile technique becomes the next priority for safe IV therapy.
What Are the Key Infection Prevention Practices for IV Insertion?
The key infection prevention practices for IV insertion include maintaining aseptic technique, changing gloves at critical steps, and assessing the site regularly. These practices reduce catheter-related infections.
How Do You Maintain Aseptic Technique Throughout IV Insertion?
You maintain aseptic technique throughout IV insertion by keeping all supplies sterile, disinfecting the insertion site thoroughly, and avoiding contact with the prepared area. Hand hygiene with alcohol-based rub or soap and water must occur immediately before catheter insertion.
Key components of aseptic technique include:
- Cleaning the site with chlorhexidine-based antiseptic in a back-and-forth friction motion and allowing it to dry completely before needle entry.
- Using only sterile, single-use catheter equipment and transparent semipermeable dressings.
- Avoiding touching the cleaned insertion area after antiseptic application.
- Performing hand hygiene again if the sterile field is compromised at any point.
According to CDC intravascular catheter infection prevention guidelines, catheter stabilization also serves as an intervention to decrease the risk for phlebitis, catheter migration, and dislodgement. Even small breaks in sterile protocol can introduce pathogens, making disciplined adherence non-negotiable for every insertion.
When Should You Change Gloves During the IV Insertion Process?
You should change gloves during the IV insertion process at specific transition points where contamination risk increases. Fresh gloves are required after patient assessment, after tourniquet application, and immediately before site disinfection and catheter insertion.
According to NCBI clinical guidance, nurses should be systematic when assessing potential vessels, examining sites both visually and through palpation while progressing from distal to proximal locations. Palpation during vein assessment inevitably contaminates gloves, so replacing them before handling sterile supplies is essential. Skipping this step is one of the most common yet preventable lapses in infection control during IV procedures.
How Often Should a Peripheral IV Site Be Assessed and Rotated?
A peripheral IV site should be assessed at least every shift (or per facility protocol) and rotated when clinically indicated. The CDC recommends replacing peripheral catheters no more frequently than every 72 to 96 hours in adults to reduce infection and phlebitis risk.
Assessment should include visual inspection and gentle palpation for:
- Redness, swelling, or tenderness suggesting phlebitis.
- Coolness, pallor, or edema indicating infiltration.
- Drainage, odor, or skin breakdown at the dressing site.
Routine replacement solely based on a fixed time schedule is no longer universally required; clinical judgment based on site condition and catheter function guides the decision. For clinicians prioritizing patient safety, treating every assessment as an opportunity to catch early complications remains the most reliable approach to reducing catheter-related infections.
What Complications Can Occur After IV Insertion and How Do You Manage Them?
Complications that can occur after IV insertion include infiltration, phlebitis, extravasation, hematoma formation, and air embolism. Each complication requires prompt recognition and a specific management approach.
How Do You Recognize and Treat IV Infiltration?
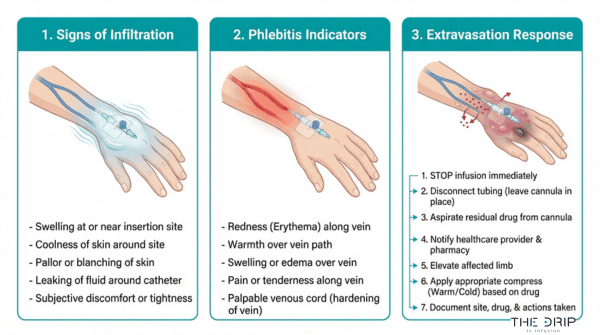
You recognize and treat IV infiltration by monitoring for swelling, coolness, and pallor at the IV site, then discontinuing the infusion immediately. Infiltration occurs when IV fluid leaks from the vein into surrounding tissue, often due to catheter dislodgement or vein wall perforation.
Key signs include:
- Localized swelling or puffiness near the insertion site
- Skin that feels cool to the touch compared to the opposite limb
- Slowed or stopped infusion flow
- Patient complaints of tightness or discomfort
To manage infiltration, stop the infusion, remove the catheter, and elevate the affected limb. Apply a warm compress for isotonic solutions or a cold compress for certain medications. Document the event and restart IV access at a new site, preferably on the opposite extremity.
What Are the Signs of Phlebitis at an IV Site?
The signs of phlebitis at an IV site are redness, warmth, tenderness, and a palpable cord along the vein path. Phlebitis is inflammation of the vein wall caused by mechanical irritation, chemical irritation from infusates, or bacterial contamination. According to the AMOR-VENUS prospective cohort study, PIVC-related phlebitis occurred in 7.5% of catheters, representing 3.3 cases per 100 catheter-days in critically ill patients.
Management steps include:
- Removing the catheter immediately upon symptom detection
- Applying warm compresses to the affected area
- Elevating the extremity to reduce swelling
- Documenting severity using a standardized phlebitis scale
- Restarting access at a new site, moving proximal on the opposite arm when possible
Phlebitis that goes unaddressed can progress to thrombophlebitis, making early identification essential for patient safety.
How Do You Identify and Respond to an Extravasation Event?
You identify and respond to an extravasation event by watching for burning pain, blistering, or tissue blanching during vesicant medication infusion, then stopping the drug immediately. Extravasation differs from infiltration because it involves the leakage of vesicant or cytotoxic agents capable of causing tissue necrosis.
Immediate response steps are:
- Stop the infusion without removing the catheter initially
- Aspirate residual medication through the catheter before removal
- Administer the appropriate antidote based on the extravasated agent
- Apply warm or cold compresses depending on the specific drug protocol
- Notify the physician and document the estimated volume of extravasate
Because tissue damage can progress over hours or days, close follow-up monitoring is critical. For most clinical teams, having an extravasation kit readily accessible prevents delays during these time-sensitive events.
What Should You Do If a Hematoma Forms During IV Insertion?
You should apply direct pressure to the site immediately if a hematoma forms during IV insertion. A hematoma develops when blood leaks into surrounding tissue, typically caused by through-and-through vein puncture or inadequate pressure after catheter removal.
To manage a hematoma effectively:
- Remove the catheter and apply firm, direct pressure for at least five minutes
- Elevate the affected extremity above heart level
- Apply a cold compress during the first 24 hours to limit swelling
- Avoid reusing the same vein or inserting distal to the hematoma site
Patients on anticoagulants or those with coagulopathies are at higher risk. For these individuals, extending pressure time to 10 minutes or longer and selecting veins with good surrounding tissue support reduces recurrence.
How Do You Manage an Air Embolism Risk During IV Therapy?
You manage an air embolism risk during IV therapy by ensuring all IV tubing is properly primed, connections are secured with Luer-lock fittings, and air is purged before line attachment. Air embolism occurs when air enters the venous system through disconnected or improperly flushed IV lines.
Prevention measures include:
- Priming all tubing completely before connecting to the patient
- Using Luer-lock connections to prevent accidental disconnection
- Positioning the patient flat or in Trendelenburg during central line access
- Clamping tubing before any disconnection or bag change
If air embolism is suspected, place the patient in the left lateral decubitus position with the head lowered. This traps air in the right ventricle and prevents it from entering the pulmonary vasculature. Administer high-flow oxygen and notify the medical team immediately.
Recognizing complications early is the foundation of safe IV practice; professional IV therapy services build these protocols into every session.
How Do You Maintain and Improve Your IV Insertion Skills Over Time?
You maintain and improve IV insertion skills through simulation training, performance tracking, and continuing education. Each approach targets a different aspect of skill development.
How Does Simulation Training Build IV Insertion Confidence?
Simulation training builds IV insertion confidence by providing repeatable, low-risk practice environments where clinicians refine technique without patient harm. Realistic manikin arms and virtual reality modules let practitioners drill vein selection, needle angle, and catheter advancement until muscle memory develops. According to a 2025 ScienceDirect meta-analysis of 15 studies, simulation-based training improved IV insertion success by 22% and reduced complications by 18%. These controlled settings also allow instructors to introduce difficult-access scenarios, helping clinicians build problem-solving skills they can transfer directly to bedside care.
Why Is Tracking Your First-Stick Success Rate Valuable?
Tracking your first-stick success rate is valuable because it creates a measurable baseline that reveals skill progression and identifies patterns behind missed attempts. A clinician who logs each insertion can pinpoint whether failures cluster around specific patient populations, catheter gauges, or vein locations. According to ESMED, first-attempt success rates for newly qualified nurses range from 44% to 76.9%, while experienced clinicians achieve 91% to 98%. That gap underscores why ongoing measurement matters; without data, improvement remains anecdotal rather than actionable.
What Continuing Education Resources Sharpen IV Insertion Technique?
Continuing education resources that sharpen IV insertion technique include peer-led simulation workshops, online procedural courses, and hands-on vascular access certification programs. According to a 2024 study published in the National Institutes of Health, simulation-based peer learning provides substantial evidence for skill improvement in procedures like IV insertion. Professional organizations also offer webinars and conference sessions covering emerging tools such as ultrasound-guided access and near-infrared vein finders. Investing in structured learning keeps clinicians current with evolving best practices and clinical standards.
How Can Professional IV Therapy Services Enhance Your Experience?
Professional IV therapy services enhance your experience by combining clinical expertise with the convenience of at-home care. The following sections cover how The Drip IV Infusion delivers mobile nurse-led IV treatments and the essential takeaways from this guide.
Can The Drip IV Infusion’s Mobile Nurses Deliver Expert IV Care at Home?
Yes, The Drip IV Infusion’s mobile nurses can deliver expert IV care at home. Founded in Fall 2022 by professionals with decades of experience in nursing, emergency medicine, and IV medical techniques, The Drip IV Infusion brings clinical-grade infusions directly to clients across Arizona. The service menu includes specialized blends for immune support, beauty enhancement, hydration, and recovery, all administered by trained nurses who apply the same evidence-based insertion techniques covered throughout this guide.
According to a 2025 Congruence Market Insights report, the global on-demand healthcare and mobile IV therapy platforms market was valued at USD 113.0 million in 2025 and is projected to reach USD 345.7 million by 2030. This rapid growth reflects increasing demand for patient-centered care delivered outside traditional clinical settings. For anyone who wants proper technique, comfort, and convenience without visiting a clinic, The Drip IV Infusion offers a practical solution.
What Are the Key Takeaways About IV Insertion Tips and Techniques?
The key takeaways about IV insertion tips and techniques center on preparation, precision, and continuous skill development. This guide covered the essential practices every clinician and patient should understand:
- Proper vein selection, catheter gauge matching, and site disinfection form the foundation of successful IV insertion.
- Techniques such as tourniquet application, warm compresses, gravity positioning, and ultrasound guidance help locate difficult veins.
- First-stick success depends on correct needle angle, skin stabilization, and palpation over visual assessment alone.
- Special populations, including pediatric, elderly, obese, and dehydrated patients, require adapted approaches for safe access.
- Avoiding common mistakes like inserting too fast, skipping the flush, or reinserting a retracted needle prevents complications.
- Pain management through topical anesthetics, distraction, and clear communication improves the patient experience.
- Infection prevention through aseptic technique, timely site rotation, and proper catheter securement reduces phlebitis and infiltration risk.
- Simulation training and tracking first-stick rates accelerate long-term skill improvement.
Mastering these fundamentals benefits both clinical professionals refining their craft and individuals seeking informed, comfortable IV therapy experiences with services like The Drip IV Infusion.