Amnioinfusion is a clinical procedure that instills sterile saline or lactated Ringer’s solution into the uterine cavity to restore amniotic fluid volume during labor. We use this guide to cover its core indications, the step-by-step procedural protocol, expected clinical outcomes, associated risks, and how it compares to other labor interventions.
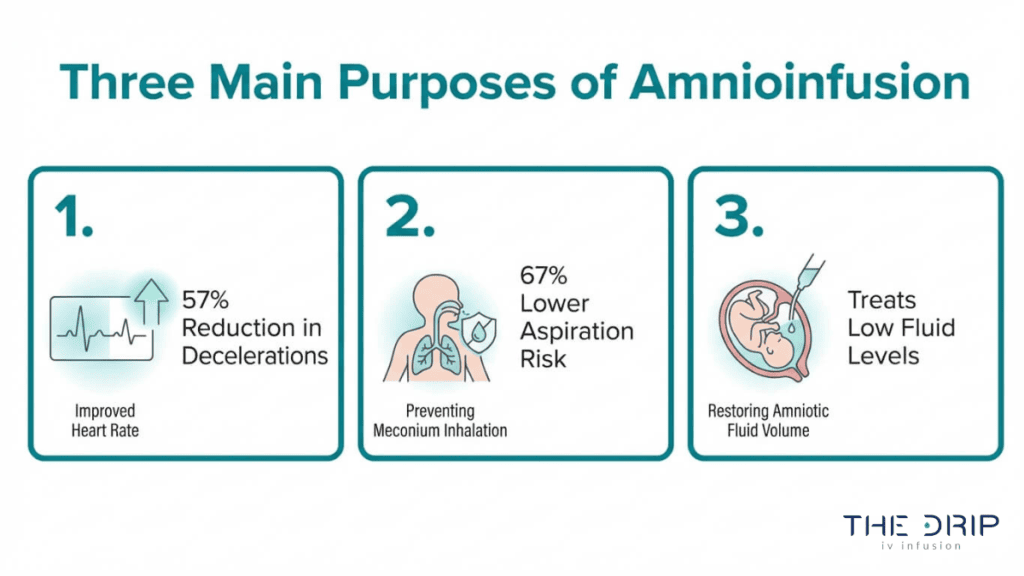
Amnioinfusion serves several primary purposes: relieving recurrent variable decelerations caused by umbilical cord compression, diluting meconium-stained amniotic fluid to lower aspiration risk, and treating oligohydramnios that leaves the fetus without adequate cushioning during contractions. ACOG recommends this procedure specifically for recurrent variable decelerations, making it one of the most targeted intrapartum tools for fetal heart rate management.
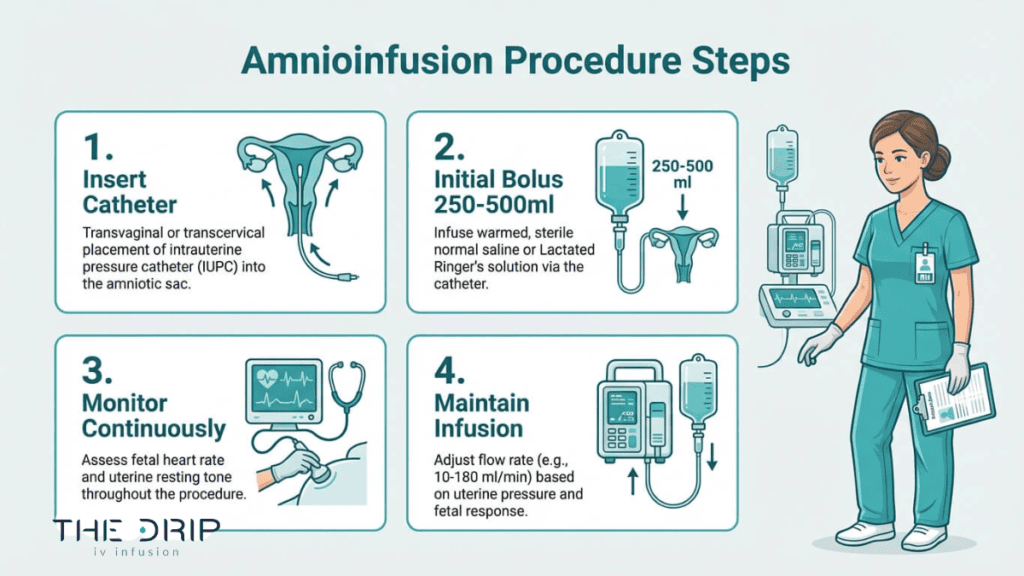
The procedure involves placing an intrauterine pressure catheter through the cervix, delivering an initial bolus of 250 to 500 ml over 20 to 30 minutes, then maintaining a continuous infusion while monitoring fetal heart rate and uterine tone in real time. Total fluid volume generally stays under 1,000 ml unless ultrasound guidance is available.
Clinical evidence shows meaningful results: a 57.4% reduction in total deceleration area, a 67% decrease in meconium aspiration syndrome odds, and an approximately 40% reduction in cesarean delivery rates when used prophylactically with meconium-stained fluid.
Complications are rare but include iatrogenic polyhydramnios, uterine hypertonus, chorioamnionitis, and amniotic fluid embolism. Contraindications such as placenta previa, placental abruption, and active infection must be ruled out before the procedure begins.
What Is the Purpose of Amnioinfusion?
The purpose of amnioinfusion is to restore amniotic fluid volume inside the uterus, protecting the fetus during labor. This procedure addresses variable decelerations, oligohydramnios, meconium-stained fluid, and umbilical cord compression.
How Does Amnioinfusion Help With Variable Decelerations?
Amnioinfusion helps with variable decelerations by restoring the fluid cushion around the umbilical cord, reducing the sudden heart rate drops triggered by cord compression during contractions. According to a study published in the International Journal of Gynecology and Obstetrics, amnioinfusion led to a 57.4% reduction in the median total deceleration area, with more substantial decreases observed in deliveries without umbilical cord entanglement.
Significant relief was documented in 68.18% of cases in the amnioinfusion group compared to only 7.1% in controls. ACOG recommends amnioinfusion specifically for recurrent variable decelerations but does not recommend it for meconium-stained amniotic fluid or preterm prelabor rupture of membranes. For clinicians weighing intervention timing, this distinction makes amnioinfusion one of the most targeted intrapartum tools available for fetal heart rate management.
How Does Amnioinfusion Treat Oligohydramnios?
Amnioinfusion treats oligohydramnios by directly replenishing the depleted amniotic fluid surrounding the fetus. When amniotic fluid levels drop dangerously low, the uterine walls press against the baby and umbilical cord, increasing the risk of fetal distress. Instilling sterile normal saline or lactated Ringer’s solution into the uterine cavity restores this protective fluid environment.
The restored volume helps normalize fetal heart rate patterns and reduces mechanical stress on the cord. While oligohydramnios can result from ruptured membranes or placental insufficiency, amnioinfusion serves as a temporary but effective measure to stabilize conditions during labor until delivery occurs.
How Does Amnioinfusion Reduce the Risk of Meconium Aspiration?
Amnioinfusion reduces the risk of meconium aspiration by diluting meconium-stained amniotic fluid, lowering the concentration of particulate matter the fetus may inhale. A meta-analysis of 24 randomized studies published in the American Journal of Obstetrics and Gynecology found that amnioinfusion reduced the overall odds of meconium aspiration syndrome by 67% (pooled odds ratio 0.33).
Beyond preventing aspiration, the procedure also resulted in a 63% decrease in neonatal intensive care unit admissions. By thinning thick meconium before it reaches the fetal airways, amnioinfusion provides a meaningful layer of protection. Given these outcomes, this intervention remains particularly valuable in settings where meconium passage is identified early in labor.
Can Amnioinfusion Prevent Umbilical Cord Compression?
Yes, amnioinfusion can prevent umbilical cord compression. The procedure instills sterile normal saline or lactated Ringer’s solution into the uterine cavity to replace lost amniotic fluid. According to a study published in the National Institutes of Health (PMC), the physiological rationale is to increase amniotic fluid volume, thereby providing a buffer that prevents the uterine walls from compressing the umbilical cord during contractions.
Without adequate fluid, each contraction forces the uterine wall directly against the cord, restricting blood flow and oxygen delivery. Amnioinfusion restores the space needed for the cord to float freely, which is why it remains a primary intervention when repeated variable decelerations suggest cord involvement during labor. Understanding amnioinfusion’s purpose helps clarify what to expect during the procedure itself.
Who Is a Candidate for Amnioinfusion?
A candidate for amnioinfusion is typically a laboring patient experiencing recurrent variable fetal heart rate decelerations or significant oligohydramnios. Specific recommendations and contraindications determine eligibility.
When Is Amnioinfusion Recommended During Labor?
Amnioinfusion is recommended during labor when recurrent variable decelerations indicate umbilical cord compression that has not resolved with standard interventions. According to the American College of Obstetricians and Gynecologists (ACOG), amnioinfusion is specifically recommended for treating recurrent variable decelerations, though ACOG does not recommend it for meconium-stained amniotic fluid or preterm prelabor rupture of membranes (PPROM).
Common clinical scenarios where providers consider amnioinfusion include:
- Persistent variable decelerations on fetal heart rate tracings despite maternal repositioning
- Documented oligohydramnios with inadequate amniotic fluid cushioning the cord
- Non-reassuring fetal heart rate patterns linked to reduced amniotic fluid volume
For most labor and delivery teams, amnioinfusion becomes a practical option only after simpler resuscitation measures, such as position changes and IV fluid boluses, have failed to resolve the concerning pattern. This sequenced approach ensures the procedure is reserved for cases where its benefits clearly outweigh the procedural requirements.
Are There Situations Where Amnioinfusion Is Not Recommended?
There are several situations where amnioinfusion is not recommended. According to the Cleveland Clinic, contraindications for amnioinfusion include an elevated uterine resting tone prior to infusion, placenta previa, placental abruption, and active intrauterine infection.
Additional conditions that preclude amnioinfusion:
- Known uterine anomalies that increase rupture risk
- Multiple gestation pregnancies where catheter placement poses added complexity
- Cases where the fetal heart rate pattern suggests an irreversible cause unrelated to cord compression
Clinicians must weigh each patient’s full obstetric picture before proceeding. A patient with a prior classical cesarean incision, for instance, carries a meaningfully different risk profile than one with an unscarred uterus. Ruling out contraindications before catheter placement protects both maternal and fetal safety.
Understanding candidacy criteria helps clarify what happens next: the step-by-step amnioinfusion procedure itself.
How Is the Amnioinfusion Procedure Performed?
The amnioinfusion procedure is performed by inserting an intrauterine catheter through the cervix and infusing sterile saline into the uterine cavity. The following subsections cover equipment, catheter placement, fluid administration, and timing.
What Equipment Is Used During an Amnioinfusion?
The equipment used during an amnioinfusion includes an intrauterine pressure catheter (IUPC), a three-way stopcock, an IV infusion pump, and sterile normal saline or lactated Ringer’s solution. According to ANMC Women’s Health Guidelines, the total volume of fluid infused should generally not exceed 1,000 ml unless ultrasound is available to titrate to an amniotic fluid index of 8 to 12 cm. Additional equipment typically includes:
- A fetal scalp electrode for continuous heart rate monitoring
- IV tubing and extension sets for fluid delivery
- Sterile drapes and gloves for infection control
Having all components assembled before the procedure begins helps clinicians respond quickly to changes in fetal status.
How Is the Intrauterine Catheter Placed?
The intrauterine catheter is placed transcervically after the amniotic membranes have ruptured. A clinician guides the IUPC through the dilated cervix and positions it alongside the fetus within the uterine cavity. Before the catheter is inserted, proper cervical dilation must be confirmed. The IUPC then measures resting uterine pressure, establishing a baseline that guides safe fluid delivery. Correct catheter positioning is essential; if the tip rests against the uterine wall or the fetus, pressure readings become unreliable and could lead to over-infusion.
How Is the Saline Solution Administered?
The saline solution is administered in two phases: an initial bolus followed by a continuous maintenance infusion. The IV bag is elevated 3 to 4 feet above the IUPC tip to create gravity-assisted flow. According to the ANMC Guideline and Procedure for Amnioinfusion, the protocol involves infusing an initial bolus of 250 to 500 ml over 20 to 30 minutes, followed by a maintenance rate of 60 to 180 ml per hour. The three-way stopcock allows clinicians to pause, adjust, or stop fluid flow without disconnecting the system. Throughout administration, uterine tone and fetal heart rate are monitored continuously.
How Long Does an Amnioinfusion Typically Take?
An amnioinfusion typically takes 20 to 30 minutes for the initial bolus, with maintenance infusion continuing throughout active labor as needed. According to the American Family Physician, a fetal scalp electrode is typically placed first, followed by an IUPC to document a resting uterine tone of less than 15 mm Hg before the infusion begins. This preparatory phase adds time before fluid delivery starts. Total duration depends on how the fetus responds; if variable decelerations resolve, the maintenance rate may be reduced or discontinued.
Understanding how amnioinfusion is performed helps clarify what to expect during fetal monitoring.
What Happens During Fetal Monitoring With Amnioinfusion?
During fetal monitoring with amnioinfusion, the clinical team continuously tracks fetal heart rate patterns and uterine activity through internal electronic monitors. An intrauterine pressure catheter (IUPC) measures resting uterine tone and contraction pressure, while a fetal scalp electrode records the baby’s heart rate in real time. Clinicians watch specifically for resolution of variable decelerations, which signal umbilical cord compression. According to the American Family Physician, a fetal scalp electrode is typically placed before initiating amnioinfusion, followed by an IUPC to document a resting uterine tone of less than 15 mm Hg. If uterine tone rises above safe thresholds or decelerations persist despite fluid infusion, the medical team may pause the procedure or pursue alternative interventions. This constant surveillance ensures that both overinfusion and inadequate response are caught early, making real-time monitoring the safety backbone of the entire amnioinfusion process. With monitoring protocols understood, the next step is evaluating the results amnioinfusion can deliver.
What Results Can You Expect After an Amnioinfusion?
Results after an amnioinfusion typically include improved fetal heart rate patterns, reduced risk of cesarean delivery, and clearer clinical decision-making. The following subsections cover response timelines, cesarean rates, and what happens when symptoms persist.
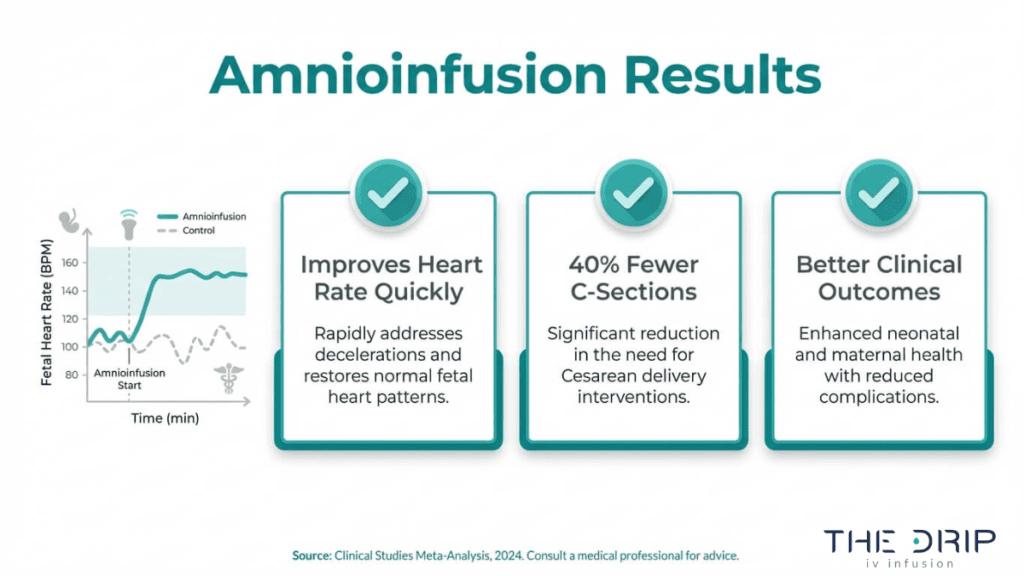
How Quickly Does Amnioinfusion Improve Fetal Heart Rate?
Amnioinfusion improves fetal heart rate patterns relatively quickly, often within the initial bolus infusion period as restored fluid volume cushions the umbilical cord. Before amnioinfusion is attempted, clinicians typically prioritize other intrauterine fetal resuscitation maneuvers, such as maternal repositioning into the left lateral decubitus position and intravenous fluid administration. Notably, according to a study published in JAMA Pediatrics, there is no evidence that maternal oxygen administration provides clinical benefit for non-reassuring fetal heart rate patterns during labor, making amnioinfusion a more targeted intervention. MFM specialists also recognize that the infused fluid provides antimicrobial factors and growth factors that assist in fetal lung expansion. Response speed depends on the underlying cause; cases without cord entanglement tend to show faster improvement.
Does Amnioinfusion Reduce the Need for Cesarean Delivery?
Amnioinfusion reduces the need for cesarean delivery in specific clinical scenarios. According to a meta-analysis published in the American Journal of Obstetrics and Gynecology, prophylactic amnioinfusion in the setting of meconium-stained amniotic fluid is associated with an approximately 40% reduction in the cesarean delivery rate (OR 0.60). This reduction stems from the procedure’s ability to resolve variable decelerations and dilute thick meconium, both of which are common triggers for emergency operative delivery. For clinicians weighing intervention options, this makes amnioinfusion one of the most practical tools for avoiding surgical delivery when cord compression or meconium is the primary concern.
What Does It Mean if Amnioinfusion Does Not Improve Symptoms?
If amnioinfusion does not improve symptoms, it typically signals that the underlying cause of fetal distress is not related to cord compression or low amniotic fluid volume. Persistent non-reassuring heart rate patterns after adequate fluid replacement may indicate placental insufficiency, uteroplacental hypoperfusion, or another etiology requiring different intervention. In these cases, the obstetric team reassesses the clinical picture and may proceed with expedited delivery, often via cesarean section. A failed response to amnioinfusion is itself valuable diagnostic information, helping clinicians narrow the cause and act decisively when continued labor poses greater risk than operative delivery.
What Are the Risks and Complications of Amnioinfusion?
The risks and complications of amnioinfusion are rare but include uterine overdistension, infection, cord prolapse, and amniotic fluid embolism. Each complication carries distinct clinical considerations.
What Is the Risk of Uterine Overdistension?
The risk of uterine overdistension during amnioinfusion involves iatrogenic polyhydramnios, a condition where excess fluid accumulates beyond what the uterus can safely accommodate. This occurs when infusion volume is not carefully monitored or titrated. Uterine hypertonus, another related complication, can develop when excessive fluid raises intrauterine pressure beyond normal resting levels. According to the ANMC Guideline and Procedure for Amnioinfusion, potential rare complications include iatrogenic polyhydramnios, uterine hypertonus, chorioamnionitis, uterine rupture, and maternal pulmonary embolus. Careful volume tracking and continuous pressure monitoring through the intrauterine catheter are essential safeguards against overdistension during the procedure.
Can Amnioinfusion Cause Umbilical Cord Prolapse?
Yes, amnioinfusion can theoretically cause umbilical cord prolapse, although the risk remains low. Cord prolapse may occur during catheter insertion or if the sudden influx of fluid displaces the umbilical cord toward the cervical os. Paradoxically, amnioinfusion is often performed specifically to relieve cord compression. The procedure restores amniotic fluid volume, which typically creates a protective cushion around the cord rather than displacing it. When the fetal presenting part is well applied to the cervix, the risk diminishes further. Continuous fetal heart rate monitoring during infusion helps clinicians detect any cord-related complications immediately, making prompt intervention possible if prolapse occurs.
What Is the Risk of Infection From Amnioinfusion?
The risk of infection from amnioinfusion centers on chorioamnionitis, an inflammation of the fetal membranes caused by bacterial contamination. Because the procedure involves inserting a catheter through the cervix into the uterine cavity, it creates a potential pathway for ascending infection. Sterile technique significantly reduces this risk. Active intrauterine infection is a contraindication for amnioinfusion, along with elevated uterine resting tone, placenta previa, and placental abruption, as noted by the Cleveland Clinic. Screening for existing infection before initiating the procedure is a critical safety step that protects both the mother and fetus.
Can Amnioinfusion Lead to Amniotic Fluid Embolism?
Amnioinfusion can, in exceedingly rare cases, lead to amniotic fluid embolism (AFE). AFE occurs when amniotic fluid enters the maternal bloodstream, triggering a severe inflammatory and coagulation response. According to a report published in the National Library of Medicine, the incidence of AFE is estimated at 2 to 8 per 100,000 maternities in the United States and United Kingdom, accounting for 5 to 15 percent of maternal deaths. While AFE is not unique to amnioinfusion and can occur during any labor, the introduction of additional fluid into the uterine cavity warrants careful monitoring. Understanding these rare but serious risks helps guide informed discussions between patients and their care teams.
How Does Amnioinfusion Compare to Other Interventions?
Amnioinfusion compares to other interventions as a targeted approach for managing non-reassuring fetal heart rate patterns, while alternatives like maternal repositioning and IV fluid boluses serve as first-line measures. Each intervention addresses fetal distress through a different mechanism.
When fetal heart rate abnormalities arise during labor, clinicians typically follow a stepwise approach. Intrauterine fetal resuscitation maneuvers often prioritize maternal repositioning, such as left lateral decubitus positioning, and intravenous fluid administration before considering amnioinfusion. These initial steps are simpler, less invasive, and require no specialized catheter placement.
Amnioinfusion differs by directly restoring amniotic fluid volume inside the uterine cavity, cushioning the umbilical cord against compression during contractions. This mechanism makes it uniquely effective for recurrent variable decelerations that persist after repositioning and fluid boluses fail.
Maternal oxygen supplementation was once a common intervention in the same clinical scenario. However, according to a study published in JAMA Pediatrics, there is no evidence that maternal oxygen administration provides clinical benefit for non-reassuring fetal heart rate patterns during labor. This finding has shifted clinical practice away from routine oxygen use during fetal distress.
The practical distinction is important: repositioning and IV fluids address maternal hemodynamics, while amnioinfusion targets the intrauterine environment itself. For clinicians managing persistent variable decelerations, amnioinfusion fills a gap that less invasive measures cannot reach.
With amnioinfusion’s role among labor interventions now clear, understanding what recovery looks like helps expecting mothers prepare for what follows delivery.
What Should Expecting Mothers Know About Amnioinfusion Recovery?
Expecting mothers should know that amnioinfusion recovery is generally straightforward because the procedure occurs during labor, and postpartum care addresses most aftereffects. Key considerations include monitoring for fluid-related complications, understanding typical post-procedure sensations, and knowing when to ask questions about the delivery outcome.
Amnioinfusion is performed as an intrapartum intervention, meaning recovery overlaps almost entirely with standard postpartum recovery. After the saline infusion ends and delivery is complete, the medical team continues monitoring uterine tone and vital signs. Most women experience no additional recovery burden beyond what normal labor and delivery require.
Because the intrauterine pressure catheter is removed after delivery, mild cramping or a sensation of increased fluid discharge is common in the hours that follow. These effects typically resolve without intervention. Nurses monitor for signs of uterine overdistension or infection during the immediate postpartum period, and any unusual symptoms like fever or persistent pain should be reported promptly.
For mothers whose amnioinfusion was performed due to variable decelerations or oligohydramnios, the neonatal team often evaluates the newborn closely after birth. Understanding why the procedure was needed helps mothers engage meaningfully with their care team during recovery. Asking about fetal heart rate response during the infusion and delivery outcomes provides clarity and reassurance.
From a practical standpoint, amnioinfusion does not extend hospital stay or require specialized post-delivery treatment. Standard postpartum protocols, including hydration, rest, and routine monitoring, apply. The most important recovery factor is open communication with the obstetric nursing staff about any concerns that arise after delivery.
How Can IV Infusion Therapy Support Maternal Wellness?
IV infusion therapy can support maternal wellness by delivering hydration and nutrients directly into the bloodstream, bypassing digestive issues common during pregnancy. The following sections cover mobile IV hydration for expecting mothers and a summary of key amnioinfusion takeaways.
Can Mobile IV Hydration Help Expecting Mothers Before and After Delivery?
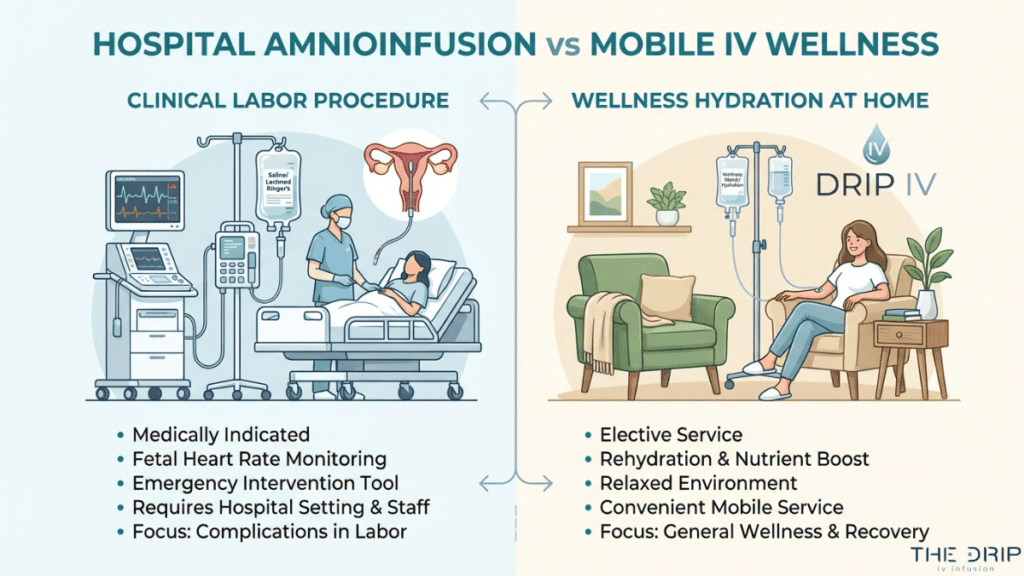
Yes, mobile IV hydration can help expecting mothers before and after delivery by providing convenient, at-home fluid replenishment. Mobile IV hydration services for expectant mothers are marketed to replace fluids lost due to morning sickness and support overall wellness during and after pregnancy. For mothers experiencing persistent nausea, oral hydration alone sometimes falls short because vomiting prevents adequate absorption.
Mobile infusions bypass the gastrointestinal tract entirely, delivering saline and selected vitamins straight to the bloodstream. The Drip IV Infusion offers mobile IV therapy specifically designed for expecting mothers dealing with morning sickness, bringing professional nursing care directly to the client’s home. However, according to a 2025 report in the American Journal of Nursing, the FDA has issued warnings to several IV infusion companies regarding the marketing of IV fluids for wellness purposes without adequate clinical evidence. Expecting mothers should always consult their healthcare provider before scheduling any IV hydration session.
What Are the Key Takeaways About Amnioinfusion We Covered?
The key takeaways about amnioinfusion covered in this article include its purpose, procedure, clinical results, and associated risks. Amnioinfusion is a hospital-based procedure that instills sterile saline into the uterine cavity to restore amniotic fluid volume during labor. Its primary indications are:
- Relieving recurrent variable decelerations caused by umbilical cord compression.
- Reducing meconium aspiration risk when meconium-stained amniotic fluid is present.
- Addressing oligohydramnios to cushion the fetus during contractions.
The procedure requires specialized equipment, including an intrauterine pressure catheter and continuous fetal monitoring. While clinical evidence supports meaningful reductions in fetal heart rate abnormalities and cesarean delivery rates, rare complications such as uterine overdistension and infection remain possible. Amnioinfusion differs entirely from wellness IV therapy; it is a clinical intervention performed by obstetric teams in labor and delivery settings. For general maternal hydration needs outside of labor, The Drip IV Infusion provides mobile IV therapy with professional nursing support.