IV fluid therapy for dehydration is a medical treatment that delivers specially formulated liquids directly into a vein to restore hydration when the body cannot rehydrate effectively through oral intake alone. The volume required ranges from as little as 0.5 liters for mild cases to 2 liters or more for severe dehydration, with precise dosing determined by severity, body weight, and clinical status.
This guide covers how IV fluid volumes are determined by dehydration severity, weight-based dosing formulas for different patient sizes, IV fluid types and their clinical applications, infusion rate guidelines, and when IV therapy becomes necessary over oral rehydration.
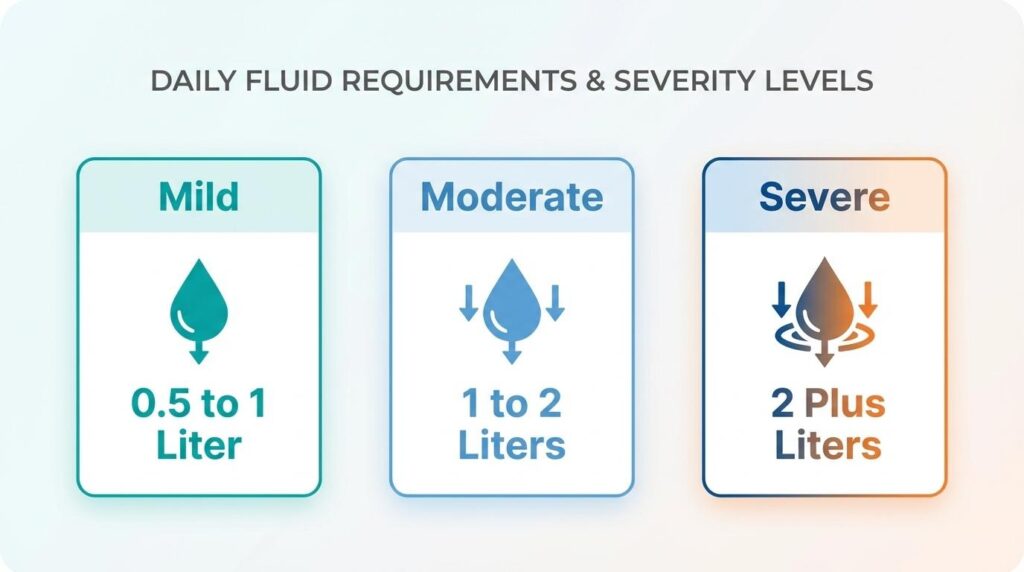
Dehydration severity is the primary factor driving IV fluid volume. Mild dehydration, representing 3% to 5% body weight loss, typically requires just 0.5 to 1 liter of isotonic crystalloid. Moderate cases escalate to 1 to 2 liters, while adults with severe hypovolemia may need 1 to 2 liters administered as rapidly as possible to restore tissue perfusion. Pediatric protocols follow age-specific schedules calculated per kilogram.
Weight-based formulas like the Holliday-Segar method and the 4-2-1 rule provide individualized dosing precision. A 70 kg adult requires roughly 1,750 to 2,100 mL daily for maintenance alone, while a 100 kg patient may need 2,500 to 3,000 mL before any deficit correction begins.
The choice between normal saline, Lactated Ringer’s, half normal saline, or D5W depends on the patient’s electrolyte balance and whether the goal is rapid volume expansion or gradual cellular rehydration. Each solution carries a distinct electrolyte profile suited to specific clinical scenarios.
Infusion speed follows the same severity logic as volume. Controlled maintenance rates work for mild cases, while severe dehydration demands aggressive bolus delivery under close monitoring to prevent both under-resuscitation and fluid overload.
What Is IV Fluid Therapy for Dehydration?
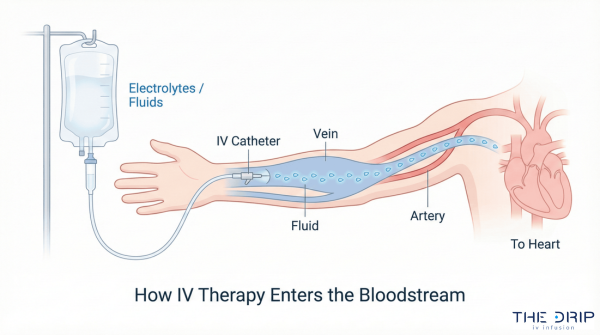
IV fluid therapy for dehydration is a medical treatment that delivers specially formulated liquids directly into a vein to restore hydration when the body cannot rehydrate effectively on its own. This method bypasses the digestive system, allowing fluids and electrolytes to reach the bloodstream immediately.
Clinicians typically reserve IV fluid therapy for situations where oral rehydration is insufficient or impractical. Severe volume depletion, persistent vomiting, and inability to tolerate fluids by mouth are common reasons a patient may need intravenous hydration instead of drinking water or electrolyte solutions. The treatment uses isotonic crystalloid solutions, such as normal saline or Lactated Ringer’s, to expand fluid volume and correct electrolyte imbalances.
Frequently asked questions about IV fluid therapy include how long a session lasts, what risks IV fluids carry, and whether IV hydration works better than drinking water. The sections that follow address these questions by covering recommended fluid volumes by dehydration severity, weight-based dosing, fluid types, and infusion rates.
How Many Liters of IV Fluid Do You Need for Dehydration?
The number of liters of IV fluid you need for dehydration depends on severity. Mild cases may require as little as 0.5 liters, while severe dehydration can demand 1 to 2 liters or more. The sections below break down volumes for mild, moderate, and severe dehydration.
How Many Liters of IV Fluid for Mild Dehydration?
The number of liters of IV fluid for mild dehydration is typically 0.5 to 1 liter of isotonic crystalloid, such as normal saline or lactated Ringer’s solution. Most clinicians consider mild dehydration a 3% to 5% loss of body weight in fluid. Oral rehydration is generally preferred at this stage, with IV therapy reserved for patients who cannot tolerate drinking fluids. When IV access is used, a single 500 mL to 1,000 mL bag administered over one to two hours is often sufficient to restore hydration. For most healthy adults experiencing mild fluid loss, this modest volume resolves symptoms like dry mouth, fatigue, and mild dizziness without overloading the cardiovascular system.
How Many Liters of IV Fluid for Moderate Dehydration?
The number of liters of IV fluid for moderate dehydration generally ranges from 1 to 2 liters in adults, adjusted by body weight and clinical response. Moderate dehydration represents approximately 6% to 9% body weight loss. According to StatPearls (NCBI Bookshelf), moderate dehydration in pediatric patients, typically representing 7% volume depletion, is managed with an initial 10 mL/kg bolus of isotonic saline without dextrose. Adults follow a similar weight-based approach, with clinicians titrating additional boluses based on vital signs and urine output. Because moderate dehydration sits at the threshold where organ function can decline, timely IV intervention prevents progression to a more dangerous stage.
How Many Liters of IV Fluid for Severe Dehydration?
The number of liters of IV fluid for severe dehydration is 1 to 2 liters or more for adults, with pediatric dosing calculated per kilogram. According to ACEP, adults in shock or with severe hypovolemia should receive 1 to 2 liters of isotonic crystalloid as quickly as possible to restore tissue perfusion. Pediatric protocols differ by age:
- Infants under 12 months receive 100 mL/kg total, divided into 30 mL/kg over 1 hour and 70 mL/kg over 5 hours.
- Children aged 12 months to 5 years receive 30 mL/kg over 30 minutes, followed by 70 mL/kg over 2.5 hours.
Once the patient’s condition stabilizes, oral rehydration can often replace continued IV therapy. Severe dehydration demands the most aggressive fluid replacement, which is why understanding body weight calculations matters next.
How Many Liters of IV Fluid Are Given Based on Body Weight?
IV fluid volumes are calculated based on body weight using standardized formulas. The sections below cover weight-based dosing for children, average adults, and larger adults.
How Much IV Fluid Does a Child Need for Dehydration?
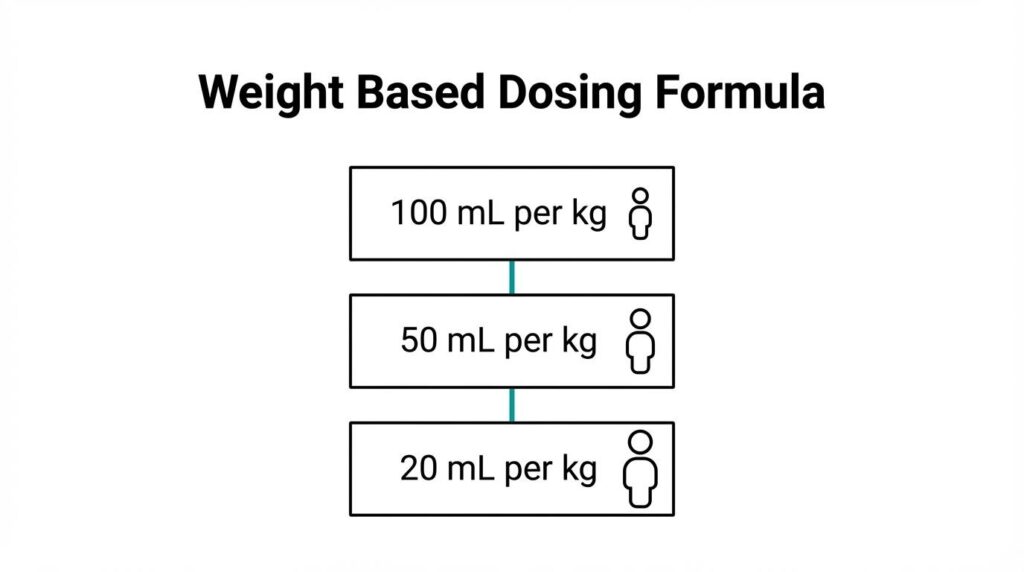
A child needs IV fluid for dehydration based on the Holliday-Segar method, which calculates maintenance requirements by weight tier. According to the Merck Manuals, this formula prescribes:
- 100 mL/kg/day for the first 10 kg of body weight
- 50 mL/kg/day for the next 10 kg
- 20 mL/kg/day for each additional kg above 20 kg
A 25 kg child, for example, would require approximately 1,600 mL (1.6 liters) per day for maintenance alone. Dehydration correction requires additional fluid beyond this baseline, calculated according to the estimated percentage of fluid loss. Clinicians often use the hourly 4-2-1 rule for infusion rate precision, applying 4 mL/kg/hr for the first 10 kg, 2 mL/kg/hr for the next 10 kg, and 1 mL/kg/hr thereafter.
How Much IV Fluid Does an Average Adult Need for Dehydration?
An average adult needs approximately 1.75 to 2.1 liters of IV fluid per day for maintenance hydration. Standard adult maintenance IV fluid requirements are approximately 25 to 30 mL per kg per day, which equates to 1,750 to 2,100 mL daily for a 70 kg adult.
For active dehydration correction, volumes increase based on severity. Mild cases may need only 1 to 1.5 liters, while moderate dehydration often requires 2 to 3 liters over several hours. Weight-based dosing ensures that a 60 kg adult receives less total volume than an 80 kg adult, even at the same dehydration level. This personalized approach reduces the risk of both under-resuscitation and fluid overload, making body weight one of the most reliable starting points for IV fluid calculations.
How Much IV Fluid Does a Large Adult Need for Dehydration?
A large adult weighing 100 kg or more needs approximately 2.5 to 3 liters of maintenance IV fluid per day. Applying the standard 25 to 30 mL/kg/day formula, a 100 kg individual requires 2,500 to 3,000 mL daily just to sustain baseline hydration.
Correcting active dehydration in larger patients demands even greater volumes, sometimes exceeding 4 liters over the first 24 hours depending on severity. However, clinicians must balance aggressive rehydration against risks like pulmonary edema or heart failure, particularly in patients with underlying cardiac or renal conditions. For most large adults without comorbidities, weight-based dosing remains the safest starting framework, with adjustments guided by urine output and clinical response.
Understanding weight-based fluid calculations helps clarify why IV formulations matter just as much as volume.
What Types of IV Fluids Are Used for Dehydration?
The types of IV fluids used for dehydration include normal saline, Lactated Ringer’s solution, half normal saline, and Dextrose 5% in Water. Each fluid has a distinct composition suited to specific clinical needs.
Normal Saline (0.9% Sodium Chloride)
Normal saline (0.9% sodium chloride) is an isotonic crystalloid solution and the most commonly used IV fluid for dehydration. According to Nurseslabs, normal saline contains 154 mEq/L of sodium and 154 mEq/L of chloride with an osmolality of 308 mOsm/L, making it the preferred choice for expanding extracellular fluid volume. Because it closely matches plasma tonicity, normal saline remains effective for initial fluid resuscitation across a wide range of dehydration scenarios. Clinicians often reach for this solution first when rapid volume expansion is the priority.
Lactated Ringer’s Solution
Lactated Ringer’s solution is a balanced isotonic crystalloid that more closely mirrors the body’s natural electrolyte composition than normal saline. As detailed by the University of Texas Medical Branch, this solution contains 130 mEq/L of sodium, 4 mEq/L of potassium, 3 mEq/L of calcium, 109 mEq/L of chloride, and lactate that the liver metabolizes to bicarbonate. That built-in buffering capacity makes Lactated Ringer’s particularly useful when metabolic acidosis accompanies dehydration, such as in cases of prolonged vomiting or diarrhea. For many rehydration scenarios, this solution offers a physiologically gentler alternative to normal saline.
Half Normal Saline (0.45% Sodium Chloride)
Half normal saline (0.45% NaCl) is a hypotonic IV solution used primarily for cellular dehydration and hypernatremia. As noted in a Taylor & Francis Group publication, this fluid should never be used for rapid fluid replacement. Its lower sodium concentration allows free water to shift into cells, gradually correcting elevated sodium levels. Clinicians typically reserve half normal saline for maintenance therapy or specific electrolyte imbalances rather than acute volume resuscitation.
Dextrose 5% in Water (D5W)
Dextrose 5% in Water (D5W) is an IV solution with a serum osmolality of 252 mOsm/L that functions as a free water source once the body metabolizes the dextrose. According to Osmosis by Elsevier, D5W becomes hypotonic after dextrose metabolism, providing free water to both extracellular and intracellular spaces. This property makes D5W suitable for treating hypernatremia and supplying modest caloric support during fluid therapy. However, because it does not provide sustained volume expansion, D5W is rarely used alone for significant dehydration.
Choosing the right fluid depends on the type and severity of dehydration; infusion speed matters just as much.
How Fast Should IV Fluids Be Administered for Dehydration?
IV fluids should be administered for dehydration at rates determined by severity, age, and clinical status. Mild to moderate cases often resolve without rapid infusion, while severe dehydration demands aggressive fluid delivery. The following sections break down recommended rates by dehydration severity.
How Fast Should IV Fluids Run for Mild to Moderate Dehydration?
IV fluids for mild to moderate dehydration should run at a controlled, moderate rate because oral rehydration is typically the preferred first-line approach. According to a CDC guideline, oral rehydration therapy is recommended as first-line therapy for mild to moderate dehydration, with IV therapy reserved for cases where oral intake fails or is contraindicated, such as intestinal ileus.
When IV fluids are necessary for mild to moderate cases, clinicians generally use maintenance-rate infusions rather than rapid boluses. Rates are calculated based on body weight, often following the 4-2-1 rule. Because the deficit is smaller, there is less urgency to push large volumes quickly; steady correction over several hours reduces the risk of fluid overload.
How Fast Should IV Fluids Run for Severe Dehydration?
IV fluids for severe dehydration should run as rapidly as clinically safe to restore perfusion. Adults in shock or with severe hypovolemia typically receive 1 to 2 liters of isotonic crystalloid as fast as possible. Pediatric protocols vary by age, with younger infants receiving boluses over slightly longer windows than older children.
A study published in the American Journal of Emergency Medicine found that rapid infusion of 50 mL/kg over 1 hour in pediatric patients was as efficacious as the same volume administered over 3 hours. This finding supports aggressive early rehydration when dehydration is severe. Clinicians monitor urine output, vital signs, and mental status throughout to confirm adequate response and adjust rates accordingly.
With infusion rates tailored to severity, recognizing when IV therapy is needed over oral rehydration becomes the next critical decision.
How Do You Know When You Need IV Fluids Instead of Oral Rehydration?
You need IV fluids instead of oral rehydration when your body cannot absorb fluids by mouth or when dehydration has become severe. The signs that indicate IV therapy is necessary fall into several categories.
According to the Cleveland Clinic, IV fluids are specially formulated liquids injected into a vein to prevent or treat dehydration, particularly when patients are unable to tolerate oral rehydration or have severe volume depletion. Recognizing the right moment to escalate from drinking fluids to receiving intravenous therapy can prevent dangerous complications.
Key indicators that IV fluids are needed instead of oral rehydration include:
- Persistent vomiting or nausea prevents you from keeping water or electrolyte drinks down long enough for absorption.
- Severe diarrhea causes fluid loss faster than oral intake can replace it.
- Altered mental status, such as confusion or extreme drowsiness, signals significant volume depletion requiring rapid intervention.
- Minimal or absent urine output over several hours suggests the kidneys are not receiving adequate fluid.
- Rapid heart rate and low blood pressure indicate the cardiovascular system is compensating for lost volume.
- Inability to swallow due to injury, surgery, or intestinal obstruction makes oral rehydration physically impossible.
Oral rehydration remains the appropriate first step for mild cases where a person can sip fluids steadily. However, once symptoms escalate to the point where the gut cannot process fluids effectively, IV therapy delivers hydration directly into the bloodstream, bypassing the digestive system entirely. For most people experiencing moderate everyday dehydration, oral solutions work well; IV fluids become essential when the body’s normal absorption pathways are compromised.
Understanding when IV therapy is warranted also helps set expectations for how the body responds once treatment begins.
What Are the Signs That IV Fluid Therapy Is Working?
The signs that IV fluid therapy is working include increased urine output, normalized vital signs, improved mental clarity, and relief from symptoms like dry mouth or dizziness. These measurable indicators help clinicians and patients confirm that rehydration is progressing effectively.
Urine output is one of the most reliable markers. According to a study from Stellenbosch University, signs of successful rehydration include a urine output of at least 0.5 mL/kg/hr in adults, normalization of vital signs, and improved mental status. A shift from dark, concentrated urine to pale yellow typically signals adequate fluid volume restoration.
Other signs that confirm effective IV fluid therapy include:
- Stabilized heart rate: A rapid pulse caused by low blood volume gradually returns to a normal resting range.
- Improved blood pressure: Hypotension from dehydration resolves as circulating volume increases.
- Restored skin turgor: Skin that previously tented when pinched returns to normal elasticity.
- Reduced thirst and dry mouth: Persistent thirst diminishes as intracellular and extracellular fluid compartments rebalance.
- Increased alertness: Confusion or lethargy associated with severe dehydration improves noticeably.
Clinicians typically reassess these parameters at regular intervals during infusion to determine whether the current rate and volume are sufficient or need adjustment. For patients receiving care outside a hospital setting, self-monitoring symptoms like energy levels, urine color, and thirst can provide practical confirmation that the therapy is delivering results. Understanding how long an IV drip typically takes helps set realistic expectations for when these improvements should appear.
How Long Does an IV Drip for Dehydration Take?
An IV drip for dehydration typically takes 30 minutes to a few hours, depending on the severity of fluid loss and the infusion rate prescribed. The timeline varies based on whether the case is mild, moderate, or severe.
For mild to moderate dehydration, a standard IV session lasts approximately 45 minutes to 1 hour. Clinicians set slower drip rates because rapid correction is unnecessary when vital signs remain stable. Many wellness and mobile IV services, including The Drip IV Infusion, complete a typical session in about 1 hour, delivering fluids at a pace that allows the body to absorb and distribute volume steadily.
Severe dehydration requires a faster approach. According to the American College of Emergency Physicians, clinicians should administer 1 to 2 liters of isotonic crystalloid as quickly as possible to restore tissue perfusion in adults with shock or severe hypovolemia. In these emergency scenarios, the initial bolus phase may take only 15 to 30 minutes before transitioning to a slower maintenance rate over several additional hours.
Several factors influence total infusion time:
- Dehydration severity: Higher fluid deficits require larger volumes and potentially faster initial rates.
- Patient weight: Heavier individuals need more total fluid, extending session length at standard drip rates.
- Fluid type: Isotonic crystalloids like normal saline or Lactated Ringer’s can be infused at varying speeds, while hypotonic solutions require slower administration.
- Clinical setting: Emergency departments can push fluids rapidly under continuous monitoring, whereas mobile or outpatient settings use controlled rates prioritizing safety.
- Patient health history: Conditions such as heart failure or kidney disease necessitate slower infusion to prevent fluid overload.
For most people seeking rehydration outside of an emergency, expecting a 45-minute to 1-hour session is reasonable. The speed of symptom relief often surprises first-time recipients, since IV delivery bypasses the gastrointestinal tract entirely. Understanding infusion timelines helps set realistic expectations, especially when considering whether excess fluid volume poses its own risks.
Can You Get Too Much IV Fluid for Dehydration?
Yes, you can get too much IV fluid for dehydration. This condition, called fluid overload or hypervolemia, occurs when the body receives more fluid than it can process. Excess IV fluid stresses the heart and lungs, potentially causing serious complications. The risks depend on infusion volume, rate, and the patient’s underlying health.
Fluid overload can develop when clinicians administer volumes beyond what a patient’s cardiovascular and renal systems can handle. Symptoms include swelling in the extremities, shortness of breath, elevated blood pressure, and rapid weight gain. Patients with heart failure, kidney disease, or liver conditions face significantly higher risk because their bodies cannot efficiently redistribute or excrete surplus fluid.
Pulmonary edema is one of the most dangerous consequences. When excess fluid accumulates in the lungs, gas exchange becomes impaired, leading to respiratory distress. Peripheral edema and electrolyte dilution, particularly hyponatremia, are also common outcomes of over-aggressive fluid resuscitation.
This is why weight-based dosing matters so much in clinical practice. Standard adult maintenance IV fluid requirements are approximately 25 to 30 mL per kg per day, according to published clinical guidelines. For a 70 kg adult, that translates to roughly 1,750 to 2,100 mL daily. Exceeding these calculated volumes without clinical justification increases the likelihood of iatrogenic fluid overload.
Proper monitoring prevents overhydration during IV therapy. Clinicians track urine output, vital signs, oxygen saturation, and physical indicators like jugular venous distension to gauge whether fluid administration should continue or slow down. Reassessment at regular intervals ensures the patient receives enough fluid to correct dehydration without tipping into excess.
For most people receiving IV hydration in a wellness or recovery setting, the risk remains low because volumes are carefully controlled. However, individuals with pre-existing cardiac, renal, or hepatic conditions should always disclose their full medical history before any infusion. Understanding both the minimum effective volume and the upper safe limit is what separates therapeutic hydration from a potentially harmful overload.
Who Is Most at Risk for Dehydration Requiring IV Fluids?
The groups most at risk for dehydration requiring IV fluids include older adults, young children, athletes, and individuals with chronic illness. Each population faces unique physiological vulnerabilities that increase fluid loss or limit oral intake.
Older adults face elevated dehydration risk due to diminished thirst response, reduced kidney function, and medication side effects such as diuretics. These factors often compound during illness or heat exposure, making oral rehydration insufficient. According to a PubMed Central study on older hospitalized patients, 62% of those admitted remained dehydrated 48 hours after admission. This persistent fluid deficit frequently necessitates IV intervention because oral intake alone cannot restore volume quickly enough. For elderly individuals managing multiple conditions, early IV fluid therapy can prevent dangerous complications like confusion, falls, and kidney injury.
Young children and infants lose fluids proportionally faster than adults due to higher metabolic rates and greater body surface area relative to weight. Vomiting and diarrhea from common childhood illnesses can escalate to moderate or severe dehydration within hours. The American Academy of Pediatrics recommends isotonic maintenance fluids, specifically 0.9% NaCl, for most hospitalized children to reduce the risk of hyponatremia. Pediatric patients who cannot tolerate oral rehydration or show signs of significant volume depletion typically require prompt IV access.
Athletes and physically active individuals lose substantial fluid and electrolytes through sweat during prolonged exertion, particularly in hot environments. When losses exceed what oral hydration can replace in time, IV fluids restore intravascular volume more rapidly. People with chronic conditions such as diabetes, kidney disease, or gastrointestinal disorders also face heightened risk because their baseline fluid balance is already compromised. Recognizing these high-risk categories early helps guide timely decisions about when IV rehydration becomes necessary over oral alternatives.
How Does Mobile IV Therapy Help With Dehydration Recovery?
Mobile IV therapy helps with dehydration recovery by delivering fluids, electrolytes, and nutrients directly into the bloodstream at the patient’s location. The following sections cover how The Drip IV Infusion provides this service at home and the key takeaways from this article.
Can The Drip IV Infusion’s Mobile Rehydration Service Treat Dehydration at Home?
Yes, The Drip IV Infusion’s mobile rehydration service can treat dehydration at home. Founded in Fall 2022 by professionals with decades of experience in nursing and emergency medicine, The Drip IV Infusion sends qualified infusion specialists directly to a client’s home or workplace in Arizona. This eliminates the need for urgent care or emergency room visits for non-emergency hydration needs.
Choosing a provider with proper medical oversight matters. According to a LinkedIn market overview, a primary restraint in the mobile IV industry is the lack of medical oversight and standardization in at-home hydration services. The Drip IV Infusion addresses this concern by staffing experienced nurses who follow established IV therapy protocols. For anyone searching for a saline drip, hydration infusion, or IV rehydration outside of a hospital, a mobile service with trained clinical staff offers a practical, accessible option.
What Are the Key Takeaways About How Many Liters of IV Fluid for Dehydration?
The key takeaways about how many liters of IV fluid for dehydration center on three factors: severity, body weight, and fluid type.
- Mild dehydration often responds to oral rehydration, while moderate cases may require 1 to 2 liters of IV fluid.
- Severe dehydration or hypovolemia can demand rapid administration of 1 to 2 liters of isotonic crystalloid to restore perfusion.
- Body weight determines precise dosing; a 70 kg adult needs approximately 1,750 to 2,100 mL daily for maintenance.
- Fluid selection, including normal saline, Lactated Ringer’s, or D5W, depends on the patient’s electrolyte status and clinical picture.
- Infusion rate matters as much as volume; faster rates are reserved for severe cases under clinical supervision.
No single answer fits every patient. The right volume depends on individual assessment by a qualified healthcare professional. For convenient, nurse-administered IV hydration at home, The Drip IV Infusion provides personalized rehydration services throughout Arizona.