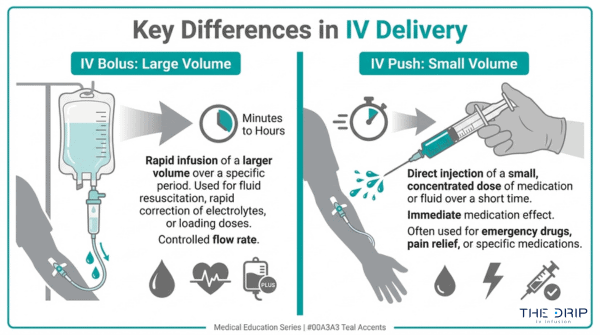
An IV bolus is a rapid, large-volume fluid delivery method, while an IV push is a small, concentrated medication injection administered directly into a vein. Both use intravenous access to bypass the digestive system, but they differ in volume, speed, purpose, and risk profile.
This guide covers how each method works, what distinguishes them clinically, the specific medications and fluids used for each, their associated risks, and how controlled IV drip infusion compares to both approaches.
IV bolus administration typically involves 250 mL to 1,000 mL of fluid delivered over several minutes to roughly 30 minutes. Clinicians use it for rapid rehydration, sepsis resuscitation, electrolyte correction, and nutrient replenishment. Common bolus fluids include normal saline, lactated Ringer’s solution, and dextrose solutions, each selected based on the patient’s condition and fluid balance needs.
IV push delivery, by contrast, involves 1 mL to 10 mL of concentrated medication injected in seconds to under one minute. Opioid analgesics, antiemetics, emergency cardiac drugs, benzodiazepines, and certain antibiotics all rely on push administration when immediate systemic drug action is required. Each drug carries specific rate guidelines; delivering too fast risks speed shock or muscle rigidity, while delivering too slow can reduce efficacy or cause paradoxical reactions.
The risk profiles reflect these differences. Bolus administration carries concerns about circulatory overload, pulmonary edema, and cardiac strain, particularly in patients with heart failure or kidney disease. Push administration poses risks of vein irritation, phlebitis, and systemic speed reactions tied to injection rate.
Healthcare providers choose between the two based on drug formulation, patient hemodynamic status, onset timing needs, and clinical setting. Controlled IV drip infusions offer a third option that prioritizes gradual, sustained absorption for wellness applications like hydration and vitamin therapy.
What Does IV Bolus Mean in Medical Terms?
An IV bolus is a rapid, large-volume injection of fluid or medication delivered directly into a vein. The subsections below cover how it is administered, what volumes qualify, and how fast delivery typically occurs.
How Is an IV Bolus Typically Administered?
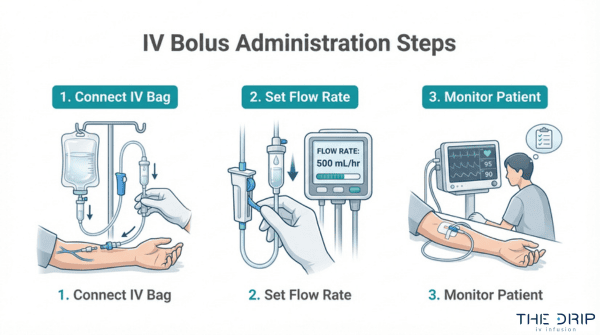
An IV bolus is typically administered by connecting a bag of fluid to a peripheral or central venous catheter and allowing it to flow at a controlled, rapid rate. A healthcare provider sets the flow based on the patient’s clinical needs, often using gravity or an infusion pump. According to StatPearls (NCBI Bookshelf), for patients with mild-to-moderate hypovolemia, fluids should be administered at a rate of 50 to 100 mL/h above estimated losses to achieve a positive fluid balance. The provider monitors vital signs throughout, adjusting the rate if the patient shows signs of intolerance. For most clinical scenarios, this method strikes a practical balance between speed and safety.
What Volume of Fluid Qualifies as an IV Bolus?
The volume of fluid that qualifies as an IV bolus depends on the clinical indication and patient weight. Sepsis resuscitation protocols, for example, often call for a standard volume of 30 mL/kg, as noted by ScienceDirect. This is substantially larger than an IV push, which involves injecting a small, concentrated amount of medication over a few seconds. However, volume must be carefully matched to the patient. In critically ill patients, fluid overload from rapid bolus administration is linked to increased mortality and complications, including pulmonary edema and cardiac failure. Clinicians must monitor closely for volume overload, especially in patients with congestive heart failure or renal failure.
How Fast Is an IV Bolus Infusion Delivered?
An IV bolus infusion is delivered within seconds to several minutes in acute clinical settings, though wellness applications may extend to 20 to 35 minutes. According to Springer Nature, an IV bolus is a rapid injection of a solution into a vein, typically completed within seconds or a few minutes, whereas continuous infusion administers medication slowly over extended periods. In acute heart failure cases, continuous infusion of loop diuretics is sometimes proposed as an alternative to bolus injection to reduce complications and achieve greater diuresis. The speed distinction matters: bolus delivery prioritizes rapid therapeutic effect, making it the preferred method when immediate fluid or medication response is critical.
With the IV bolus defined, understanding IV push administration reveals how these two methods differ in practice.
What Does IV Push Mean in Medical Terms?
IV push is a method of delivering medication directly into the bloodstream through a vein, typically in under one minute. The following subsections cover how it is administered, what volume qualifies, and how fast the injection is delivered.
How Is an IV Push Typically Administered?
An IV push is typically administered by a healthcare provider who injects a small, concentrated dose of medication directly into a vein or an existing IV line over a short period, often less than one minute. According to the National Center for Biotechnology Information (NCBI), intravenous push is the process of introducing a medication or fluid substance directly into the bloodstream via the venous system.
Administration speed varies by drug. Morphine, for instance, should be delivered over 4 to 5 minutes and diluted to reduce respiratory depression risk. Atropine, by contrast, requires rapid delivery because slow administration may cause paradoxical bradycardia. This drug-specific variability makes IV push one of the most technique-sensitive methods in intravenous therapy.
What Volume of Medication Qualifies as an IV Push?
The volume of medication that qualifies as an IV push is typically a small, concentrated amount, usually ranging from 1 to 10 mL per dose. Because volumes are small, precise concentration standardization becomes critical for patient safety. ASHP’s Standardize 4 Safety initiative addresses this directly as a national effort to standardize medication concentrations and reduce errors across different administration routes, including IV push.
Given how little fluid is involved, even minor dosing miscalculations can significantly affect patient outcomes. Practitioners should always verify drug-specific concentration guidelines before delivering any IV push medication.
How Fast Is an IV Push Injection Delivered?
An IV push injection is delivered over a range of a few seconds to five minutes, depending on the specific medication. Most IV push drugs are administered in under one minute, though certain agents require slower delivery to prevent adverse reactions.
Even with appropriate technique, some risk of local irritation exists. A study published in PMC found that rapid IV push administration of 500 mg thiamine was associated with injection site reactions in 0.86% of doses. While this incidence is low, it reinforces the importance of following drug-specific rate guidelines for every IV push medication.
Understanding push delivery mechanics sets the stage for comparing how IV bolus and IV push differ in speed.
How Do IV Bolus and IV Push Differ in Speed?
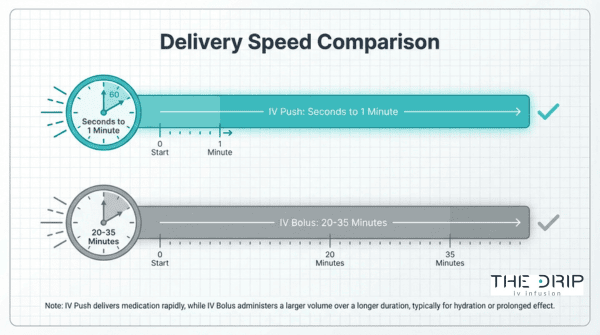
IV bolus and IV push differ in speed primarily by timeframe: an IV push delivers medication in seconds to under one minute, while an IV bolus completes delivery over several minutes to roughly 30 minutes. The distinction matters because administration rate directly affects how the body absorbs and responds to intravenous substances.
An IV push is the faster method. According to the National Center for Biotechnology Information, intravenous push introduces a medication or fluid substance directly into the bloodstream via the venous system, typically in less than one minute. This near-instantaneous delivery makes IV push ideal for emergency cardiac drugs and acute pain management, where even brief delays can compromise patient outcomes.
An IV bolus, while still considered rapid compared to continuous infusion, operates on a longer timeline. Delivery can be completed in approximately 20 to 35 minutes depending on the volume and clinical context. That broader window allows larger fluid volumes to enter the circulatory system without overwhelming venous pressure.
The speed difference carries clinical significance beyond convenience:
- IV push speed (seconds to under 1 minute) enables immediate drug action for time-sensitive interventions.
- IV bolus speed (minutes to roughly 30 minutes) allows controlled delivery of larger volumes for hydration or nutrient replenishment.
- Continuous infusion speed (hours) maintains steady-state drug levels over extended periods.
Faster is not always better. Administering certain substances too rapidly through an IV push can trigger speed shock, a systemic reaction involving chest pressure, irregular pulse, and potential cardiac arrest. For most wellness and hydration scenarios, the slightly slower bolus pace provides a safer, more comfortable experience while still delivering results far faster than oral alternatives.
How Do IV Bolus and IV Push Differ in Volume?
IV bolus and IV push differ in volume primarily by scale: bolus delivery involves larger fluid volumes, while push delivery uses small, concentrated medication doses. The distinctions below clarify typical ranges and why volume matters clinically.
IV bolus volumes typically range from 250 mL to 1,000 mL of fluid, though resuscitation protocols may call for even larger amounts. Sepsis guidelines, for example, often specify 30 mL/kg as a standard fluid bolus volume. These larger volumes serve purposes such as rapid rehydration, electrolyte correction, and circulatory support. Because the fluid load is substantial, clinicians must monitor patients closely for signs of volume overload, particularly in those with compromised cardiac or renal function.
IV push volumes, by contrast, rarely exceed 10 mL per injection. Most IV push medications are delivered in concentrated doses of 1 mL to 5 mL, injected directly into the vein or through an existing IV line. According to the AHRQ Patient Safety Network, the compact volume of IV push medications demands precise syringe technique, since even small miscalculations in concentration can produce outsized pharmacological effects. This is why standardization efforts like ASHP’s Standardize 4 Safety initiative focus on consistent medication concentrations across care settings.
The volume difference between these two methods carries direct clinical consequences:
- Fluid balance impact: Bolus volumes shift overall fluid status, making them unsuitable for patients prone to pulmonary edema or heart failure.
- Concentration risk: Push volumes are small but highly potent, so delivery speed and dilution accuracy become the primary safety concerns.
- Equipment requirements: Bolus delivery often uses IV bags with gravity drip or infusion pumps, while push delivery requires only a syringe and a patent IV access point.
- Monitoring priorities: Bolus administration demands hemodynamic monitoring for fluid tolerance; push administration demands observation for immediate drug reactions.
For clinicians and patients alike, recognizing that volume dictates both the delivery method and the risk profile is essential when choosing between these two approaches. Understanding these volume distinctions helps clarify why each method suits different therapeutic goals.
How Do IV Bolus and IV Push Differ in Purpose?
IV bolus and IV push differ in purpose based on whether the clinical goal requires volume replacement or rapid medication delivery. The subsections below cover when each method is preferred.
When Is an IV Bolus Preferred Over an IV Push?
An IV bolus is preferred over an IV push when the clinical goal requires large-volume fluid delivery for hydration, resuscitation, or nutrient replenishment. Situations involving dehydration, blood pressure stabilization, or electrolyte correction call for the sustained volume that bolus infusions provide.
Bolus administration also reduces the risk of speed shock, a systemic reaction characterized by chest pressure, irregular pulse, and cardiac arrest that can occur when a substance enters the bloodstream too rapidly via IV push, according to Pressbooks’ Nursing Advanced Skills resource. Because bolus infusions distribute larger fluid volumes over a longer window, they allow the body to absorb nutrients and fluids gradually without the concentrated vascular impact of a direct push.
When Is an IV Push Preferred Over an IV Bolus?
An IV push is preferred over an IV bolus when a patient needs immediate systemic medication effects in a small, concentrated dose. Emergency scenarios requiring rapid drug onset, such as cardiac arrest intervention or acute pain management, rely on push delivery because it places the full medication concentration into the bloodstream within seconds.
IV push is also preferred for drugs that lose efficacy when diluted in larger fluid volumes. Medications requiring precise, time-sensitive dosing benefit from the controlled syringe technique that push administration provides. For patients who cannot tolerate high fluid volumes due to heart failure or renal impairment, push delivery achieves the therapeutic goal without adding circulatory fluid burden. Understanding these purpose-driven distinctions helps clarify which medication types are best suited for each method.
What Types of Medications Are Given by IV Push?
The types of medications given by IV push include opioid analgesics, antiemetics, emergency cardiac drugs, benzodiazepines, and rapid-acting antibiotics. Each drug class has specific rate requirements to balance therapeutic speed with patient safety.
Opioid Analgesics
Opioid analgesics such as morphine and fentanyl are commonly delivered by IV push for rapid pain control. According to the New Jersey Health Care Coalition’s adult and pediatric IV push medication reference, morphine administered via IV push should be delivered over 4 to 5 minutes and may be diluted to a final concentration of 0.5 to 5 mg/mL to reduce the risk of respiratory depression. Fentanyl requires administration over 1 to 2 minutes because rapid delivery can cause skeletal muscle and chest wall rigidity. Precise rate control makes IV push the preferred route when immediate analgesia is critical, particularly in emergency and post-surgical settings.
Antiemetics
Antiemetics are medications that suppress nausea and vomiting, and several are routinely given by IV push. Ondansetron (Zofran) is one of the most widely used options in this class. According to a UNC Health adult quick IV push reference, ondansetron for post-operative nausea and vomiting should be administered via IV push over at least 30 seconds, though 2 to 5 minutes is preferred. This controlled injection rate helps prevent headache and QT prolongation. For patients who cannot tolerate oral dosing, IV push antiemetics provide reliable absorption that bypasses the gastrointestinal tract entirely.
Emergency Cardiac Drugs
Emergency cardiac drugs such as atropine, adenosine, and epinephrine rely on IV push for life-saving speed during cardiac events. Atropine is a particularly instructive example: it should be administered as a rapid IV push because slow administration may cause paradoxical bradycardia rather than the intended heart rate increase, as noted in Vizient’s IV medication administration guidelines. This paradoxical response underscores why rate specifications vary by drug class. In cardiac arrest and unstable arrhythmias, even seconds of delay can affect outcomes, making IV push the standard delivery route for frontline resuscitation medications.
Benzodiazepines
Benzodiazepines are sedative medications frequently given by IV push to manage seizures, acute anxiety, and procedural sedation. Diazepam, lorazepam, and midazolam each have specific push rates, typically ranging from 1 to 2 minutes depending on the agent. Slow, controlled delivery is essential because overly rapid injection increases the risk of respiratory depression and hypotension. Lorazepam, often the first-line choice for status epilepticus, requires careful rate monitoring despite the urgency of seizure termination. This balance between speed and safety makes benzodiazepines one of the drug classes where IV push technique directly influences clinical outcomes.
Rapid-Acting Antibiotics
Rapid-acting antibiotics are given by IV push when infections require immediate therapeutic drug levels in the bloodstream. Agents such as ceftriaxone, cefazolin, and certain penicillin derivatives can be administered over 2 to 5 minutes via direct injection. This approach is common in emergency departments where bacterial infections present with acute symptoms like sepsis or meningitis. Not all antibiotics qualify for push delivery; many require slower infusion to avoid adverse reactions like red man syndrome or phlebitis. Clinicians select IV push antibiotics based on the drug’s stability profile and the patient’s clinical urgency, reserving this method for agents proven safe at rapid injection rates.
With specific push medications in context, the fluids used for IV bolus administration serve a different clinical purpose.
What Types of Fluids Are Given as an IV Bolus?
The types of fluids given as an IV bolus include normal saline, lactated Ringer’s solution, and dextrose solutions. Each serves a distinct clinical purpose based on the patient’s condition.
Normal Saline
Normal saline is a 0.9% sodium chloride solution and the most widely used crystalloid for IV bolus administration. Clinicians rely on it for rapid volume resuscitation, dehydration correction, and as a compatible carrier for many IV medications. According to a 2016 study published in BMC Nephrology, intravenous fluid administration in the ICU requires differentiating between maintenance, replacement, and resuscitative therapies to select appropriate crystalloids like normal saline or lactated Ringer’s. Its balanced sodium content closely mirrors blood plasma concentration, making it a versatile first-line choice in emergency and routine settings alike.
Lactated Ringer’s Solution
Lactated Ringer’s solution is a balanced crystalloid containing sodium, potassium, calcium, and lactate. It more closely resembles the body’s extracellular fluid composition than normal saline. Clinicians often prefer it for surgical patients, trauma resuscitation, and burn recovery because its buffered formulation helps reduce the risk of hyperchloremic metabolic acidosis. When large-volume boluses are needed, this balanced electrolyte profile makes lactated Ringer’s a particularly practical option over prolonged fluid replacement.
Dextrose Solutions
Dextrose solutions are glucose-based IV fluids used as a bolus to address hypoglycemia or provide caloric support. The most common formulations include 5% dextrose in water (D5W) and 10% dextrose (D10W). D5W delivers a modest glucose supply while contributing free water for hydration, whereas D10W provides a more concentrated caloric source for patients with critically low blood sugar. Because dextrose is metabolized quickly, these solutions are often combined with saline or electrolyte bases when sustained volume expansion is also needed.
With fluid types established, understanding the risks of each IV administration method helps guide safer clinical decisions.
What Are the Risks of IV Push Administration?
The risks of IV push administration include speed shock, vein irritation, and local injection site reactions. These complications relate directly to how fast the medication enters the bloodstream and the chemical properties of the drug itself.
What Happens if an IV Push Is Delivered Too Quickly?
If an IV push is delivered too quickly, the patient risks a dangerous systemic reaction known as speed shock. Speed shock is characterized by chest pressure, irregular pulse, and potential cardiac arrest when a foreign substance enters the bloodstream too rapidly, according to Nursing Advanced Skills (Pressbooks). Certain medications carry unique fast-injection risks; fentanyl, for example, can trigger skeletal muscle and chest wall rigidity if not administered over the recommended one to two minutes. This is why drug-specific rate guidelines exist for nearly every IV push medication. Clinicians who rush the process trade seconds of convenience for potentially life-threatening consequences.
Can IV Push Medications Cause Vein Irritation?
Yes, IV push medications can cause vein irritation, most commonly presenting as phlebitis. A study reported by The Cardiology Advisor found that phlebitis is the most common complication of peripheral intravenous access, occurring in 44% of cases, followed by infiltration at 16.3% and occlusion at 7.6%. Concentrated medications delivered through small peripheral veins are particularly prone to triggering this inflammatory response. Even nutrients considered generally safe carry measurable risk when pushed intravenously; IV push thiamine at 500 mg doses was associated with injection site reactions in 0.86% of administrations. Proper vein selection, adequate dilution, and controlled push rates all help reduce local irritation significantly.
Understanding push-specific risks clarifies why bolus administration carries its own distinct concerns.
What Are the Risks of IV Bolus Administration?
The risks of IV bolus administration include circulatory overload, pulmonary edema, and cardiac strain from rapid fluid delivery. The following subsections cover system overload consequences and populations who should avoid large-volume boluses.
What Happens if an IV Bolus Overloads the Circulatory System?
An IV bolus overloads the circulatory system when fluid volume exceeds the heart’s ability to pump effectively, causing a dangerous rise in venous pressure. This excess fluid forces plasma into surrounding tissues and lung spaces. According to a study published in PMC (National Institutes of Health), fluid overload from rapid bolus administration in critically ill patients is linked to increased mortality and complications such as pulmonary edema and cardiac failure.
Common signs of circulatory overload include:
- Sudden shortness of breath and oxygen desaturation
- Elevated jugular venous pressure
- Peripheral edema in the extremities
- Rapid, bounding pulse with rising blood pressure
Even in non-critical settings, clinicians must monitor fluid input closely. Smaller, measured boluses with reassessment between doses reduce the chance of pushing the cardiovascular system past its compensatory limits.
Who Should Avoid Receiving a Large-Volume IV Bolus?
Patients with pre-existing cardiovascular or renal conditions should avoid receiving a large-volume IV bolus without careful clinical oversight. Fluid boluses for sepsis patients often involve a standard volume of 30 mL/kg; however, according to a ScienceDirect study on sepsis fluid resuscitation, clinicians must carefully monitor for volume overload in patients with congestive heart failure or renal failure.
High-risk populations include:
- Patients with congestive heart failure, where excess volume worsens cardiac output
- Individuals with chronic kidney disease who cannot excrete fluid efficiently
- Elderly patients with reduced cardiac reserve and lower tolerance for rapid volume shifts
- Neonates and pediatric patients with smaller total blood volumes
For anyone considering IV therapy outside a hospital, this is precisely why provider screening matters before any fluids are administered.
How Do Healthcare Providers Decide Between IV Bolus and IV Push?
Healthcare providers decide between IV bolus and IV push by evaluating the medication’s pharmacological profile, the required volume, the patient’s clinical stability, and the urgency of the situation. The key decision factors include drug-specific protocols, patient risk assessment, and the clinical setting where treatment occurs.
Choosing the wrong method carries real consequences. Medication errors for drugs given intravenously have some of the highest error rates in healthcare, estimated between 48% and 53% in hospital and long-term care settings, according to SingleCare’s medication error analysis. This makes proper method selection a critical patient safety concern, not merely a procedural preference.
Healthcare providers typically weigh several factors before selecting a delivery method:
- Drug formulation requirements: Some medications require rapid systemic delivery via IV push, while others need the larger fluid volumes that IV bolus provides.
- Patient hemodynamic status: Patients with compromised cardiac or renal function may not tolerate the rapid volume shifts associated with bolus administration.
- Onset timing needs: Emergency situations often demand IV push for near-instant drug action, whereas fluid resuscitation calls for bolus delivery.
- Vein condition and access quality: Concentrated IV push medications can increase irritation risk in fragile or small-gauge peripheral lines.
- Clinical setting and scope of practice: The expansion of IV treatments in medical spa and mobile settings requires protocols that ensure healthcare providers work within their appropriate clinical scope to maintain safety, as noted in the American Journal of Nursing.
For most clinical decisions, the medication itself dictates the method. Drugs with narrow therapeutic windows or known speed-related complications almost always have manufacturer-specified administration rates that remove guesswork from the equation. When providers follow these drug-specific guidelines alongside individualized patient assessment, the risk of administration errors drops significantly.
Understanding these clinical decision points helps clarify why IV therapy protocols exist and how each delivery method serves a distinct therapeutic purpose within the broader spectrum of intravenous treatment.
How Does IV Drip Infusion Compare to Both IV Bolus and IV Push?
IV drip infusion compares to both IV bolus and IV push primarily through its controlled, slower delivery rate. The Infusion Nurses Society provides evidence-based standards guiding clinical decisions across all three methods. The subsections below clarify how a controlled drip differs from a bolus and from a push.
What Makes a Controlled IV Drip Different from a Bolus?
A controlled IV drip differs from a bolus in delivery speed and volume regulation. An IV bolus delivers a large fluid volume rapidly, sometimes within minutes, to restore hydration or correct deficits quickly. A controlled IV drip, by contrast, uses gravity or a programmable pump to administer fluids steadily over 30 to 60 minutes or longer.
This slower rate reduces the risk of circulatory overload, making drip infusions safer for patients who cannot tolerate sudden fluid shifts. Bolus delivery prioritizes speed; drip infusion prioritizes sustained, gradual absorption. For most wellness applications, the controlled drip strikes a better balance between efficiency and comfort.
What Makes a Controlled IV Drip Different from a Push?
A controlled IV drip differs from a push in volume, duration, and clinical intent. IV push delivers a small, concentrated medication dose directly into the vein, often in under one minute. A controlled drip administers a larger solution containing fluids, vitamins, or minerals over a prolonged period.
Because push injections enter the bloodstream almost instantly, they carry a higher risk of speed-related reactions. Drip infusions dilute active ingredients across a steady flow, reducing vein irritation and systemic shock risk. For nutrient-based therapies like hydration or vitamin delivery, controlled drips offer gentler, more sustained absorption than either bolus or push methods.
Understanding these distinctions helps when choosing the right IV therapy approach for your goals.
How Should You Approach IV Therapy with Mobile IV Infusion Services?
You should approach IV therapy with mobile IV infusion services by verifying provider credentials, understanding which delivery method suits your needs, and confirming that safety protocols align with clinical standards. The following sections cover how customized IV cocktails compare to clinical methods and the key takeaways from this guide.
Can The Drip IV Infusion’s Customized IV Cocktails Deliver the Same Benefits as Clinical IV Methods?
Yes, The Drip IV Infusion’s customized IV cocktails can deliver the same core benefits as clinical IV methods because they use the same intravenous delivery mechanism that bypasses the GI tract for maximum absorption. Mobile IV therapy provides medical-grade hydration and nutrient therapy directly to patients’ locations, with services often including health screenings via telehealth before administration.
The Drip IV Infusion employs nurses with decades of experience in emergency medicine, home health, and IV medical techniques. Each session uses proven blends of vitamins, minerals, and hydration fluids administered through controlled infusion protocols.
What separates a quality mobile provider from a clinical setting is not the delivery science; it is the customization. The Drip IV Infusion builds each IV cocktail around individual health goals, offering add-ons such as glutathione, Vitamin C, zinc, and NAC to tailor every treatment.
What Are the Key Takeaways About IV Bolus vs Push?
The key takeaways about IV bolus vs push center on three distinctions: volume, speed, and clinical purpose.
- IV bolus delivers larger fluid volumes over minutes, making it ideal for rapid hydration, fluid resuscitation, and nutrient replenishment.
- IV push injects small, concentrated medication doses directly into the vein within seconds, suited for time-sensitive drug delivery.
- Speed and volume determine risk profiles; bolus carries fluid overload concerns while push carries speed shock risks.
- Healthcare providers select between bolus and push based on patient condition, medication properties, and desired onset time.
- Safety protocols from organizations like the Infusion Nurses Society guide clinical decision-making for both administration methods.
According to ISMP, programmable infusion pumps with dose error-reduction systems should be used for all medication and hydration infusions to minimize administration errors. Understanding these differences helps you ask better questions before any IV treatment, whether in a hospital or through a mobile service like The Drip IV Infusion.