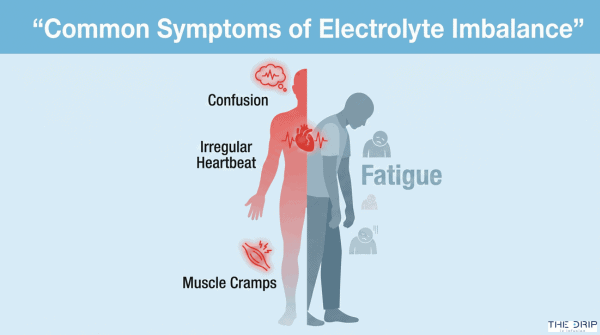
If you’re experiencing symptoms like muscle cramps, fatigue, confusion, or irregular heartbeat, you might be dealing with an electrolyte imbalance. We understand how concerning these symptoms can be, especially when they interfere with your daily life. You’re in the right place to learn about one of the most effective medical interventions for restoring your body’s delicate electrolyte balance—IV therapy.
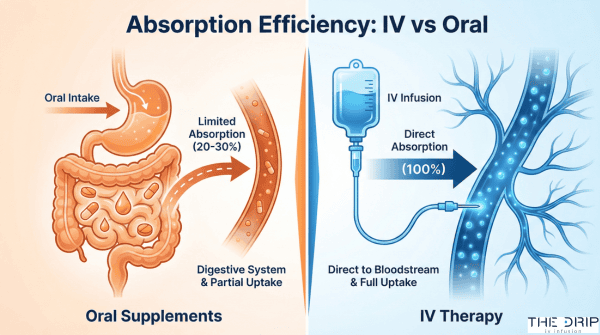
Intravenous (IV) therapy for electrolyte imbalance is a medical treatment that delivers essential minerals like sodium, potassium, calcium, and magnesium directly into your bloodstream through a vein, achieving up to 100% absorption compared to only 20-30% with oral supplements. This direct delivery method rapidly corrects dangerous imbalances that affect 34.4% of critically ill patients for hyponatremia, 29.0% for hypokalemia, and 26.7% for hypocalcemia.
TL;DR Summary:
• Electrolyte imbalances occur when minerals in your blood fall outside normal ranges, causing symptoms from mild fatigue to life-threatening cardiac arrhythmias, with diagnosis confirmed through blood tests showing levels like sodium below 135 mmol/L or potassium below 3.6 mmol/L.
• IV therapy works by delivering balanced crystalloid solutions containing precise electrolyte concentrations directly into your bloodstream, with options like Lactated Ringer’s (sodium 130 mmol/L, potassium 4.0 mmol/L) or Normal Saline (sodium and chloride 154 mmol/L each).
• Medical conditions requiring IV therapy include severe dehydration, sepsis (where balanced solutions reduce mortality from 29.4% to 25.2%), diabetic ketoacidosis, pancreatitis, and situations where oral intake is impossible.
• Common side effects include phlebitis (39.25% cumulative incidence) and infiltration (15.7-33.8% of IV catheters), though serious complications remain rare with proper monitoring and technique.
• Post-therapy maintenance involves gradual tapering of IV fluids, regular electrolyte monitoring, dietary adjustments, and preventive measures to reduce future imbalance risks.
• The Drip IV Infusion provides professional mobile IV therapy services throughout Pinellas and Hillsborough counties with licensed medical staff, no travel fees, and FSA/HSA acceptance.
Quick Tip: If you’re receiving IV therapy at home or in a clinic, ensure your provider uses the smallest gauge needle that accommodates your prescribed therapy—this simple step significantly reduces your risk of complications like phlebitis and infiltration.
Understanding how IV therapy corrects electrolyte imbalances empowers you to make informed decisions about your treatment options. In the following sections, we’ll explore the science behind electrolyte imbalances, examine how different IV solutions work, identify who benefits most from this therapy, discuss potential risks, and provide practical guidance for maintaining healthy electrolyte levels after treatment.
What Are Electrolyte Imbalances and Why Do They Matter?
Electrolyte imbalances are disruptions in the body’s mineral concentrations that regulate critical functions such as nerve signaling, muscle contraction, and fluid balance. These imbalances require immediate medical attention because they can lead to cardiac arrhythmias, seizures, and organ failure. The following sections examine the causes, symptoms, and diagnostic methods for identifying electrolyte disturbances requiring IV therapy intervention.
What Causes Electrolyte Imbalances in the Body?
The primary causes of electrolyte imbalances are fluid loss from decreased intake, surgery, vomiting, diarrhea, and diaphoresis. Severe dehydration occurs through vomiting, diarrhea, fever, and heat exhaustion, creating urgent need for electrolyte replacement. Medical conditions causing significant disruption include diabetic ketoacidosis, sepsis, pancreatitis, and traumatic blood loss.
Gastrointestinal losses deplete sodium and potassium rapidly. Kidney dysfunction impairs the body’s ability to regulate mineral levels. Endocrine disorders such as adrenal insufficiency affect multiple electrolyte systems simultaneously.
Understanding these causes helps medical professionals determine appropriate IV therapy protocols for restoration.
What Are the Most Common Symptoms of Electrolyte Imbalances?
The most common symptoms of electrolyte imbalances are neurological changes, muscle dysfunction, and cardiac irregularities. Hyponatremia manifests as headaches, confusion, nausea, delirium, and neurological deterioration. Hypernatremia presents with tachypnea, sleeping difficulty, and restlessness.
Potassium imbalances create distinct patterns. Hypokalemia causes weakness, fatigue, muscle twitching, and hypokalemic paralysis. Hyperkalemia leads to muscle cramps, weakness, rhabdomyolysis, myoglobinuria, and cardiac arrhythmias.
A 2021 critical care study found hyponatremia in 34.4%, hypokalemia in 29.0%, and hypocalcemia in 26.7% of critically ill patients. These prevalence rates highlight the importance of systematic electrolyte monitoring in hospital settings.
How Are Electrolyte Imbalances Diagnosed?
Electrolyte imbalances are diagnosed through serum blood tests measuring specific mineral concentrations. Hyponatremia occurs at serum sodium levels below 135 mmol/L. Hypernatremia develops when serum sodium exceeds 145 mmol/L. Hypokalemia manifests at serum potassium below 3.6 mmol/L. Hyperkalemia appears when serum potassium surpasses 5.5 mmol/L.
Calcium disorders require corrected measurements. Hypocalcemia exists at corrected serum total calcium below 8.8 mg/dL. Hypercalcemia occurs when corrected serum total calcium exceeds 10.7 mg/dL.
Point-of-care testing devices enable rapid electrolyte assessment from small blood samples. The i-STAT 1 system and epoc Blood Analysis System provide results within minutes. The cobas b 123 POC system delivers fully automated blood gas and electrolyte analysis.
These diagnostic tools allow immediate identification of imbalances requiring IV therapy correction, preparing patients for the targeted electrolyte replacement protocols discussed in the following section.
How Does IV Therapy Work to Restore Electrolyte Balance?
IV therapy works to restore electrolyte balance by delivering precise concentrations of minerals directly into the bloodstream through intravenous administration. This method bypasses the digestive system entirely, achieving immediate correction of electrolyte deficiencies. Medical professionals administer crystalloid solutions containing sodium, potassium, calcium, and magnesium at therapeutic concentrations. The following sections explore the specific electrolytes delivered, safety protocols, and effectiveness compared to oral methods.
What Types of Electrolytes Are Delivered Via IV Therapy?
The types of electrolytes delivered via IV therapy include sodium, potassium, calcium, magnesium, and chloride in precisely formulated concentrations. Normal plasma reference values guide these formulations: sodium 135-145 mmol/L, potassium 4.5-5.0 mmol/L, calcium 2.2-2.6 mmol/L, and magnesium 0.8-1.0 mmol/L.
| Solution | Sodium (mmol/L) | Potassium (mmol/L) | Calcium (mmol/L) | Magnesium (mmol/L) |
| Lactated Ringer | 130 | 4.0 | 1.5 | – |
| Normal Saline | 154 | – | – | – |
| Plasmalyte | 140 | 5.0 | – | 1.5 |
| Ringer Acetate | 145 | 4.0 | 2.5 | 1.0 |
Crystalloids remain the most commonly used IV solutions due to availability, low cost, and minimal allergic reaction risk. Each solution offers unique electrolyte profiles matching specific clinical needs.
How Is the IV Therapy Process Administered Safely?
The IV therapy process is administered safely through smart infusion pumps, standardized protocols, and continuous monitoring. According to 2024 data, 87.1% of infusions use smart pumps integrated with EMR systems for real-time monitoring. The 2024 Infusion Therapy Standards of Practice provides 66 standards with over 2,500 references guiding safe administration.
Safety measures include:
- Using the smallest gauge cannula accommodating prescribed therapy
- Diluting irritant medications like vancomycin and potassium chloride
- Administering hypertonic saline (3% solution) through central lines only
- Limiting correction rates to 0.5 mEq/hour to prevent osmotic demyelination
- Conducting regular IV site assessments
- Replacing cannulas timely
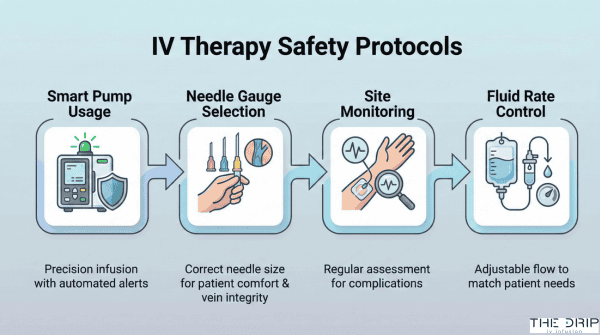
These protocols minimize complications while ensuring therapeutic effectiveness.
What Makes IV Therapy More Effective Than Oral Rehydration for Electrolyte Correction?
IV therapy is more effective than oral rehydration for electrolyte correction because it achieves up to 100% nutrient absorption compared to 20-30% with oral therapy. Treatment failure rates demonstrate this superiority: 0.7% for IV therapy versus 4.6% for oral rehydration in pediatric populations. For every 25 children treated orally, one requires IV rescue therapy.
IDSA guidelines recommend IV fluids for specific conditions including infectious diarrhea with shock, severe dehydration, altered mental status, or ileus. Fluid bolus effects from IV therapy last approximately 120 minutes, providing rapid stabilization. Patients unable to take medications orally require IV administration for effective correction. This direct delivery method ensures predictable therapeutic outcomes when oral intake proves inadequate or impossible.
Who Can Benefit Most from IV Therapy for Electrolyte Imbalance?
IV therapy delivers critical electrolytes directly into the bloodstream for patients who cannot maintain proper mineral balance through oral intake alone. Medical conditions ranging from sepsis to severe dehydration create urgent needs for intravenous electrolyte replacement, while specific patient populations require careful evaluation before treatment.
What Medical Conditions Make IV Electrolyte Replacement Necessary?
Medical conditions that make IV electrolyte replacement necessary include sepsis, diabetic ketoacidosis, pancreatitis, hyponatremia, severe dehydration, and malnutrition. A 2018 meta-analysis in the New England Journal of Medicine found sepsis patients receiving balanced crystalloids experienced in-hospital mortality of 25.2% compared to 29.4% with saline (n=15,802). Diabetic ketoacidosis patients treated with lactated Ringer solution show faster resolution times and earlier insulin discontinuation according to 2022 emergency medicine guidelines.
| Condition | Clinical Finding | Source |
| Sepsis | 4.2% mortality reduction with balanced crystalloids | NEJM 2018 |
| Hyponatremia | Affects 28.8% of hospitalized patients | Clinical Medicine 2019 |
| Pancreatitis | Reduced ICU admissions with lactated Ringer therapy | Gastroenterology 2021 |
| Severe dehydration | Requires immediate IV replacement for GI losses | IDSA 2023 |
Hyponatremia occurs in 28.8% of hospitalized patients and associates with extended hospital stays. Severe gastrointestinal fluid losses from vomiting or diarrhea require immediate IV intervention when oral replacement fails.
When Is IV Therapy Recommended Over Other Treatments?
IV therapy is recommended over other treatments when oral intake becomes impossible due to altered mental status, ileus, severe hypovolemia, or shock. The 2023 Infectious Diseases Society of America guidelines specify IV fluids for patients with infectious diarrhea presenting with shock, severe dehydration, or inability to tolerate oral fluids. Severe hypovolemia and shock demand immediate intravenous resuscitation to restore circulating volume.
Cerebral edema management requires specific IV protocols with careful fluid selection to prevent worsening brain swelling. A 2022 critical care study found major adverse kidney events occurred in 14.3% of patients receiving balanced crystalloids versus 15.4% with normal saline (n=15,802). Conservative fluid management after initial resuscitation reduces complications such as pulmonary edema, acute respiratory distress syndrome, and acute kidney injury.
For stable patients who can tolerate oral intake, oral rehydration therapy may show comparable effectiveness with hospital stays averaging 1.2 days shorter than IV therapy.
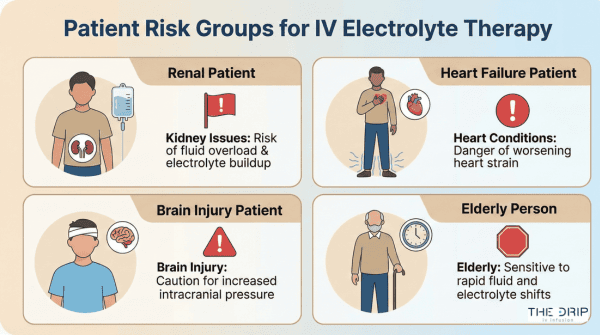
Are There Any Groups Who Should Avoid IV Electrolyte Therapy?
Groups who should avoid or use caution with IV electrolyte therapy include renal dialysis patients, heart failure patients, traumatic brain injury patients, and elderly individuals. Renal dialysis patients cannot process large fluid volumes due to impaired kidney function, making continuous IV fluids contraindicated. Heart failure patients face increased fluid overload risk requiring careful monitoring during any IV administration.
A 2021 traumatic brain injury study revealed higher mortality with balanced solutions (19.1%) compared to saline (14.7%) in this population (n=8,616). Burn injury patients may benefit more from dextrose and normal saline combinations rather than lactated Ringer alone based on 2020 burn care guidelines.
| Patient Group | Consideration | Clinical Impact |
| Renal dialysis | Contraindicated for continuous fluids | Renal impairment prevents processing |
| Heart failure | Increased fluid overload risk | Requires careful monitoring |
| Traumatic brain injury | Higher mortality with balanced solutions | 19.1% vs 14.7% with saline |
| Elderly patients | Increased fluid overload risk | Special monitoring needed |
Patients with diabetes mellitus, chronic kidney disease, or peripheral vascular disease show no worse outcomes compared to healthy individuals when receiving appropriate IV electrolyte therapy. These findings prepare healthcare providers to identify candidates who benefit most from IV intervention while recognizing populations requiring modified approaches.
What Are the Potential Risks and Side Effects of IV Electrolyte Therapy?
The potential risks and side effects of IV electrolyte therapy include phlebitis, infiltration, and local infection. Phlebitis occurs with a cumulative incidence of 39.25% and median onset time of 5 days. Infiltration affects 15.7% to 33.8% of IV catheters. Local infection rate is 0.150% with incidence of 65.1 per 100,000 catheter-days. Understanding these risks helps patients and providers optimize treatment safety. The following sections detail patient expectations, risk minimization strategies, and warning signs requiring immediate intervention.
What Should Patients Expect During and After IV Therapy?
Patients should expect that 50% of peripheral IVs will fail during their treatment course. Infiltration affects 15.7% to 33.8% of IV catheters, with a mean rate of 23.9%. Upper extremity involvement accounts for 89.6% of infiltration events. Superficial soft tissue infection, including cellulitis and thrombophlebitis, occurs in 8.6% of infiltrations. Phlebitis develops with a cumulative incidence of 39.25% and median onset time of 5 days. Local infection rate remains relatively low at 0.150% with an incidence of 65.1 per 100,000 catheter-days. These complications may manifest as pain, swelling, or redness at the IV site during or after treatment completion.
How Can Adverse Reactions to IV Electrolyte Correction Be Minimized?
Adverse reactions to IV electrolyte correction can be minimized by avoiding high-risk factors and following specific administration protocols. Female sex increases phlebitis risk with an adjusted hazard ratio of 1.58. Using 18-gauge cannulas doubles phlebitis risk with a hazard ratio of 2.02. Potassium chloride administration increases phlebitis risk by 93%. Vancomycin administration nearly triples phlebitis risk with a hazard ratio of 2.89.
Healthcare providers should avoid cannulation of flexion sites unless clinically justified. Eight medications, including ciprofloxacin, diazepam, and propofol, should be given through a separate line from lactated Ringer solution. Post-infusion phlebitis monitoring should extend 48-96 hours after catheter removal to catch delayed reactions.
What Are the Warning Signs That Require Immediate Medical Attention?
The warning signs that require immediate medical attention are tissue death, wound formation, and vascular complications. Necrosis or eschar formation occurs in 3.2% of infiltration cases. Ulceration or full-thickness wound formation develops in 1.9% of infiltrations. Compartment syndrome, though rare at 0.0% in recent studies, requires emergency intervention when suspected. Deep vein thrombosis occurs in 0.2% of infiltration cases.
High-volume normal saline infusion may cause hyperchloremic metabolic acidosis. Central line-associated bloodstream infections occur at 1.7 per 1,000 central line days in ICUs. Patients experiencing severe pain, numbness, color changes, or systemic symptoms should seek immediate medical evaluation to prevent permanent complications.
How Can You Maintain Healthy Electrolyte Levels After IV Therapy?
Maintaining healthy electrolyte levels after IV therapy requires careful monitoring and gradual dietary adjustments. The transition from IV support to normal intake demands systematic assessment of fluid status and electrolyte balance. Post-therapy management focuses on preventing rebound imbalances while supporting the body’s natural regulation mechanisms.
What Dietary and Lifestyle Changes Support Electrolyte Balance?
Dietary and lifestyle changes that support electrolyte balance include gradual tapering of IV fluids as patients resume normal diet and fluid intake. Healthcare providers monitor skin turgor, urinary output, lung sounds, and oxygen requirements continuously during this transition period. Fluid boluses should be avoided unless the patient shows clear volume depletion signs. Daily input/output balance tracking prevents progressive volume overload, which occurs when fluid administration exceeds the body’s elimination capacity.
The transition period requires careful attention to dietary sodium, potassium, and magnesium intake through whole foods. Patients benefit from consuming electrolyte-rich foods such as bananas, spinach, avocados, and yogurt while limiting processed foods high in sodium. Adequate hydration through regular water intake supports kidney function and electrolyte regulation. These dietary modifications work alongside clinical monitoring to maintain stable electrolyte levels after IV therapy discontinuation.
How Often Should Electrolyte Levels Be Monitored for Ongoing Health?
Electrolyte levels should be monitored regularly post-therapy, with frequency determined by initial imbalance severity and patient response. Continuous monitoring of fluid and electrolyte status remains essential during the immediate post-therapy period. Healthcare providers evaluate the ongoing need for replacement fluids through serial laboratory assessments and clinical evaluation. New edema development indicates fluid management issues requiring immediate attention and potential therapy adjustment.
A 2021 clinical review in Critical Care Medicine found that patients with severe initial imbalances require daily monitoring for 72 hours post-therapy, followed by weekly assessments for one month. Stable patients may transition to monthly monitoring after demonstrating consistent normal values. Assessment parameters include serum sodium, potassium, calcium, and magnesium levels alongside clinical signs such as mental status changes, muscle weakness, or cardiac rhythm abnormalities.
Are There Preventive Measures to Reduce the Risk of Future Imbalances?
Preventive measures to reduce future imbalance risk include frequent monitoring of IV sites for high-risk drugs and implementation of standardized electrolyte administration protocols. Regular staff training on IV therapy protocols reduces adverse events by ensuring consistent best practices. Healthcare facilities implementing standardized protocols report decreased complication rates and improved patient safety outcomes. Passive leg raise tests and noninvasive cardiac output measurements accurately determine fluid responsiveness without invasive procedures.
According to a 2023 Joint Commission study on IV therapy safety, institutions with quarterly staff training programs showed 42% fewer electrolyte-related adverse events compared to those with annual training only. Prevention strategies also include patient education about recognizing early imbalance symptoms, maintaining adequate hydration, and following prescribed dietary modifications. Regular follow-up appointments allow early detection and intervention before severe imbalances develop, supporting long-term electrolyte stability after IV therapy completion.
How Does The Drip IV Infusion Support Effective Electrolyte Correction?
The Drip IV Infusion supports effective electrolyte correction through licensed medical professionals who deliver mobile IV therapy services directly to patients across Pinellas, Hillsborough, and surrounding areas. This locally-owned service emphasizes precision in electrolyte replacement through specialized drips targeting specific imbalance conditions.
Why Should You Consider The Drip IV Infusion for IV Therapy Needs?
The Drip IV Infusion for IV therapy needs offers distinct advantages through its mobile service model and professional medical staff. Licensed nurses and paramedics administer treatments with clinical precision. The company maintains a no-travel-fee policy while accepting FSA/HSA payments for accessibility.
Specialized services address common electrolyte imbalance causes:
• Stomach Bug Relief Drip for gastrointestinal fluid losses
• Immunity & Wellness Drip for preventive electrolyte support
• Energy & Performance Drip for athletic recovery
• Hangover Relief Drip for alcohol-related dehydration
Mobile IV therapy eliminates transportation barriers for patients experiencing severe symptoms. The service brings hospital-grade electrolyte correction directly to homes, offices, or hotels throughout the service area.
What Are the Key Takeaways About IV Therapy for Correcting Electrolyte Imbalance?
The key takeaways about IV therapy for correcting electrolyte imbalance include significant mortality reduction and market growth indicators. A 2023 BEST-Living Study meta-analysis of 34,685 patients demonstrates balanced crystalloid solutions reduce mortality by 4% relative to normal saline. This translates to saving one life per 250 patients treated.
Insurance coverage typically applies when IV therapy meets medical necessity criteria. The global IV therapy market reached $2.3 billion valuation in 2023 with projections reaching $4.9 billion by 2033.
Clinical outcomes favor balanced solutions over normal saline:
• Major adverse kidney events: 4.7% with balanced crystalloids vs 5.6% with saline
• Treatment duration: continued until vital signs normalize
• Tissue perfusion: monitored until mental status improves
• Ileus resolution: required before therapy discontinuation
These evidence-based outcomes support The Drip IV Infusion’s approach to personalized electrolyte correction through targeted IV formulations and professional administration protocols.