If you’re concerned about elevated blood urea nitrogen (BUN) levels, you’re likely seeking clear information about how IV fluid therapy can help restore kidney function and improve your health outcomes. We understand the anxiety that comes with abnormal lab results, and we’re here to provide you with comprehensive, evidence-based guidance on this important treatment option.
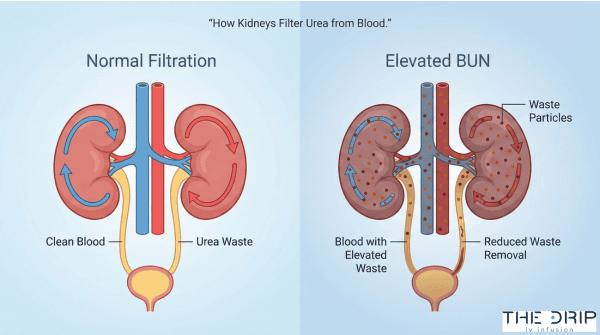
Elevated BUN levels indicate that your kidneys may not be functioning optimally to filter waste products from your blood. Blood urea nitrogen is a waste product created when your body breaks down proteins, and when levels rise above the normal range of 8-20 mg/dL, it signals potential kidney dysfunction or dehydration that requires medical attention.
TL;DR Summary: This guide covers everything you need to know about IV fluid therapy for high BUN levels. We explain how different IV fluids work to restore kidney function through improved blood flow and filtration. We detail when IV therapy is indicated based on specific lab values and symptoms, particularly when the BUN/creatinine ratio exceeds 20:1. We discuss the types of fluids used, with balanced crystalloids showing superior outcomes compared to normal saline. We outline what to expect during treatment, including typical dosing of 10-20 mL/kg administered as a bolus and monitoring parameters like urine output targets of >30 mL/hour. We address potential complications like fluid overload and when IV therapy should be avoided. Finally, we explore alternatives including diuretic therapy and renal replacement options, plus lifestyle strategies for maintaining healthy BUN levels long-term.
Quick Tip: If you’re experiencing symptoms of dehydration along with elevated BUN levels, drinking water alone may not be sufficient—IV fluids can restore your body’s fluid balance within 24 hours when administered properly, potentially preventing the need for more intensive treatments like dialysis.
What Causes High BUN Levels and Why Is It a Concern?
High BUN levels occur when kidneys cannot effectively filter waste products from blood. Blood urea nitrogen (BUN) measures the amount of nitrogen in blood from urea, a waste product of protein metabolism. According to Medscape clinical guidelines, normal BUN range is 8-20 mg/dL. Values above this threshold indicate impaired kidney function or increased protein breakdown.
The primary causes of elevated BUN include dehydration, kidney disease, heart failure, gastrointestinal bleeding, and high protein intake. Prerenal causes account for most cases, particularly when the BUN/Creatinine ratio exceeds 20:1, indicating reduced blood flow to kidneys or increased protein catabolism. The following sections examine specific risk factors and health impacts of elevated BUN.
What Are the Most Common Risk Factors for Elevated BUN Levels?
The most common risk factors for elevated BUN levels are dehydration, chronic kidney disease, heart failure, and acute kidney injury. A 2013 global burden study found acute kidney injury reached 13.3 million cases worldwide, with 85% occurring in low-income or lower-middle-income countries.
Azotemia, the medical term for elevated BUN, accounts for up to 16% of hospitalized patients globally. Risk factors include:
- Advanced age and diabetes mellitus
- Hypertension and cardiovascular disease
- Nephrotoxic medications such as NSAIDs, aminoglycosides, and contrast agents
- Severe infections and sepsis
- Volume depletion from vomiting, diarrhea, or burns
A BUN/Creatinine ratio greater than 20:1 indicates prerenal causes or increased protein catabolism. This ratio helps distinguish between prerenal azotemia (reduced kidney perfusion) and intrinsic kidney disease.
How Does High BUN Affect the Body’s Health?
High BUN affects the body’s health by increasing mortality risk and indicating kidney dysfunction. Patients with BUN ≥7.30 mmol/L show higher in-hospital mortality rates of 3.3% versus 0.5% (P<0.001) compared to those with normal levels.
Critically ill patients in the top BUN quartile (>27 mg/dL) have nearly 70% higher 30-day mortality. Elevated BUN constitutes an independent predictor of mortality in ICU patients, separate from other kidney function markers.
| Patient Group | BUN Level | Mortality Impact |
| Acute Ischemic Stroke | Elevated | 45% higher 90-day mortality |
| Acute Ischemic Stroke | Elevated | 36% higher 180-day mortality |
| ICU Patients | >27 mg/dL | 70% higher 30-day mortality |
| Hospitalized | ≥7.30 mmol/L | 3.3% vs 0.5% in-hospital |
High BUN levels may cause uremic symptoms including nausea, fatigue, confusion, and metallic taste. These symptoms result from accumulation of toxic waste products normally cleared by healthy kidneys. Understanding these health impacts guides treatment decisions for IV fluid therapy and other interventions.
How Do IV Fluids Work to Lower High BUN Levels?
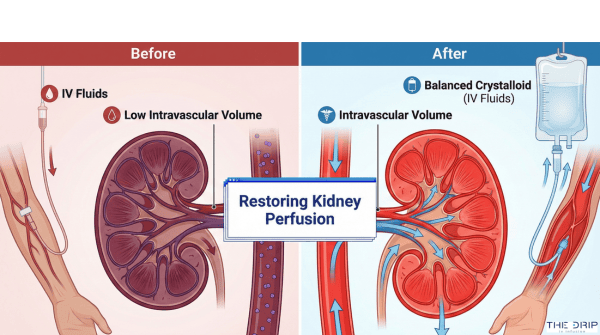
IV fluids work to lower high BUN levels by restoring intravascular volume, improving kidney perfusion, and enhancing the glomerular filtration rate. When dehydration or volume depletion causes prerenal azotemia, crystalloid solutions rapidly expand blood volume and trigger the release of atrial natriuretic peptide. According to a 2021 AAFP clinical guideline, fluid resuscitation reverses prerenal azotemia within 24 hours in dehydration cases. The following subsections detail the specific fluid types, kidney function improvements, and mechanisms through which IV therapy reduces elevated BUN.
What Types of IV Fluids Are Used for High BUN Reduction?
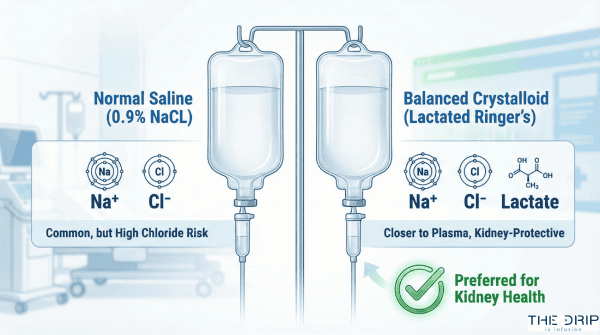
The types of IV fluids used for high BUN reduction are isotonic crystalloids, with balanced solutions preferred over normal saline. Normal saline (0.9% NaCl) contains 154 mEq/L sodium and 154 mEq/L chloride. Balanced crystalloids such as Lactated Ringer’s and Plasma-Lyte A demonstrate superior renal outcomes compared to normal saline.
According to 2022 AAFP guidelines, isotonic crystalloids are recommended over colloids as initial therapy. A 2020 meta-analysis found no significant difference in AKI incidence between crystalloids and colloids (OR 1.03, 95% CI 0.89-1.18). Albumin may be reserved for refractory cases when hypoalbuminemia contributes to volume instability.
The selection between fluid types depends on patient-specific factors and chloride content considerations for optimal kidney protection.
How Does IV Fluid Therapy Improve Kidney Function?
IV fluid therapy improves kidney function through acute intravascular volume expansion and enhanced renal perfusion. Bolus infusion triggers release of atrial natriuretic peptide, which increases renal blood flow and promotes natriuresis. A 2018 study on chloride-restrictive strategies found balanced crystalloids showed lower AKI incidence and reduced need for renal replacement therapy.
According to a 2019 trial on critically ill patients, balanced crystalloids demonstrated improved composite renal outcomes with absolute risk reduction of 1.1% (NNT=91). The mechanism involves restoration of effective circulating volume, which directly enhances glomerular filtration.
These physiological improvements occur rapidly when appropriate fluid selection and administration protocols are followed.
What Is the Mechanism by Which IV Fluids Remove Excess BUN?
The mechanism by which IV fluids remove excess BUN involves restoration of circulating volume and improved glomerular filtration rate. Crystalloids administered in boluses (300 mL every 2 hours) show better outcomes in acute tubular necrosis compared to slow hydration. A 2020 study on ATN management confirmed bolus infusion is preferred over continuous slow hydration.
IV fluids restore kidney perfusion by expanding intravascular volume and reducing renal vasoconstriction. According to 2021 clinical data, fluid resuscitation reverses prerenal azotemia within 24 hours in dehydration cases. The enhanced filtration allows kidneys to clear accumulated urea nitrogen more effectively.
Understanding these mechanisms helps healthcare providers optimize fluid therapy protocols for patients with elevated BUN levels requiring immediate intervention.
When Is IV Fluid Therapy Indicated for High BUN Levels?
IV fluid therapy is indicated for high BUN levels when volume depletion, prerenal azotemia, or shock causes kidney dysfunction. Healthcare providers assess specific symptoms, laboratory markers, and clinical findings to determine fluid resuscitation needs while screening for contraindications like heart failure or fluid overload.
What Symptoms or Lab Results Signal the Need for IV Fluids?
The need for IV fluids is signaled by a BUN/creatinine ratio ≥15 in acute ischemic stroke patients requiring saline hydration. Oliguria or anuria from shock requires immediate crystalloid bolus therapy. Volume depletion with elevated BUN/Cr ratio >20:1 suggests prerenal azotemia that responds to fluid resuscitation. Mean arterial pressure below 65 mm Hg serves as the acceptable threshold for initiating fluid therapy. These laboratory and clinical markers guide healthcare providers in identifying patients who may benefit from IV fluid administration for elevated BUN levels.
Who Should Not Receive IV Fluid Treatment for High BUN?
Patients who should not receive IV fluid treatment include those with heart failure requiring fluid restriction rather than additional fluids. Cardiorenal disease with existing fluid overload contraindicates IV fluid therapy. Pulmonary edema risk prevents aggressive fluid resuscitation in susceptible patients. Severe hypoalbuminemia may require colloids rather than standard crystalloids for volume expansion. These contraindications highlight the importance of individualized assessment before initiating IV fluid therapy for high BUN levels.
How Is the Need for IV Fluids Determined by Healthcare Providers?
The need for IV fluids is determined through NICE guidelines’ ABCDE approach for assessing hypovolemia and fluid resuscitation requirements. Healthcare providers apply the KDIGO 2012 AKI guidelines’ risk stratification approach to guide therapy decisions. Integration of kidney function measures including BUN, creatinine, and urine output provides comprehensive assessment data. Early nephrology consultation within 48 hours benefits complex cases requiring specialized management. This systematic evaluation ensures appropriate patient selection for IV fluid therapy while avoiding unnecessary treatment in those who may not benefit or could experience harm from fluid administration.
What Are the Risks, Side Effects, and Alternatives to IV Fluids for High BUN?
The risks, side effects, and alternatives to IV fluids for high BUN include fluid overload complications, diuretic therapies, and renal replacement options. IV fluid therapy carries risks of pulmonary edema and electrolyte imbalances while alternatives like furosemide or continuous renal replacement therapy offer different approaches for managing elevated BUN levels.
What Potential Complications Are Associated with IV Fluid Therapy?
The potential complications associated with IV fluid therapy are fluid overload, pulmonary edema, cardiovascular strain, interstitial edema, and chloride-related acid-base disturbances. Fluid overload leads to endothelial dysfunction through inflammation and ischemia-reperfusion injury. Pulmonary edema and cardiovascular overload represent major complications of excessive IV fluid administration.
Interstitial edema impairs oxygen and metabolite diffusion while increasing tissue pressure. Excess chloride from normal saline may worsen renal function and cause acid-base disturbances. A 2014 meta-analysis on early goal-directed therapy (EGDT) found longer ICU stays versus usual care with a mean difference of 2.81 days (95% CI 0.21-5.41).
What Other Treatments Can Help Lower High BUN Without IV Fluids?
Other treatments that can help lower high BUN without IV fluids are high-dose furosemide, the “tank and blast” approach, continuous renal replacement therapy, ultrafiltration, and oral rehydration. High-dose IV furosemide (100-160 mg) may be administered after 2L fluids with no urine output improvement. The “tank and blast” approach combines continuous noradrenaline (0.06-0.12 μg/kg/min) plus furosemide (10-30 mg/hr).
Continuous renal replacement therapy (CRRT) decreases BUN from 127 to 74 mg/dL according to clinical studies. Ultrafiltration serves as a safe alternative to diuretics in heart failure and cardiorenal syndrome patients. Oral rehydration is non-inferior to IV hydration in moderate CKD patients, offering a less invasive option.
How Do the Benefits of IV Fluids Compare to Other Methods?
The benefits of IV fluids compared to other methods show no difference in 90-day mortality between early versus delayed renal replacement therapy in septic shock. A study comparing early RRT (within 12 hours) versus delayed RRT (48 hours) found no mortality difference in septic shock patients. Diuretics are not recommended for AKI treatment or prevention except for volume overload management.
The RenalGuard system, which uses furosemide-induced diuresis with matched hydration, shows the best outcomes with a SUCRA score of 0.974. Hemodynamic guided hydration ranks second best for contrast-induced AKI prevention with a SUCRA score of 0.849. These specialized systems may offer advantages over standard IV fluid protocols in specific clinical scenarios.
What Should You Expect During and After IV Fluid Treatment for High BUN?
IV fluid treatment for elevated BUN levels involves precise administration protocols and careful monitoring. The treatment process follows established clinical guidelines with specific dosing, timing, and assessment parameters. Healthcare providers track multiple indicators to evaluate treatment response and adjust therapy accordingly.
What Happens During an IV Fluid Infusion Session?
An IV fluid infusion session begins with the administration of crystalloid solutions at calculated doses based on body weight and clinical condition. The standard fluid resuscitation dose is 10-20 mL/kg administered as a bolus. According to NICE guidelines, healthcare providers administer a 500 mL crystalloid bolus over less than 15 minutes for acute resuscitation needs.
Hemorrhagic shock patients receive larger volumes, with crystalloids given as 1-2 liter boluses to restore circulating volume rapidly. For ongoing fluid needs, maintenance fluids follow the Holliday-Segar formula: 4 mL/kg/hr for the first 10 kg of body weight, allowing precise fluid replacement tailored to individual metabolic requirements.

How Soon Will BUN Levels Respond to IV Fluids?
BUN levels typically show measurable changes within hours of initiating IV fluid therapy. Resolution of azotemia is expected within 24 hours from fluid therapy initiation in dehydration cases. However, rapid BUN decreases may indicate severe kidney dysfunction—a decrease of more than 33% in the first 12 hours associated with a twofold elevated risk of dialysis or death.
Treatment response guides further interventions. If no response occurs to the “tank and blast” approach within 6 hours, dialysis or continuous renal replacement therapy (CRRT) should be considered. In stroke patients, BUN/creatinine ratio improvements correlate with better functional outcomes at 72 hours, demonstrating the prognostic value of early response patterns.
How Is Progress Monitored After IV Fluid Therapy?
Progress monitoring after IV fluid therapy relies on multiple clinical parameters to assess treatment effectiveness. Urine output serves as the primary indicator, with targets of greater than 30 mL/h in shock resuscitation and 30-50 mL/hour in burn resuscitation. Healthcare teams monitor serum BUN, creatinine levels, and the BUN/creatinine ratio through serial blood tests.
Volume status assessment includes tracking weight changes, blood pressure measurements, and capillary refill time. Follow-up scheduling depends on recovery speed: patients with renal function recovered to 90% or more from baseline require follow-up at 3 months. Slower recovery cases need earlier follow-up at 3 weeks, then again at 3 months to ensure continued improvement and detect any complications.
These monitoring protocols ensure safe, effective treatment while identifying patients who may need alternative therapies or specialist consultation for optimal outcomes.
How Can Lifestyle, Diet, and Hydration Affect BUN Levels?
Lifestyle, diet, and hydration directly affect BUN levels through their impact on kidney function and protein metabolism. Proper hydration maintains glomerular filtration rate while dietary protein intake determines nitrogen waste production. Managing these factors prevents BUN elevation and supports kidney health long-term.
What Dietary Changes Help Manage BUN Levels?
Dietary changes that help manage BUN levels include reducing protein intake, limiting sodium, and increasing plant-based foods. High protein diets increase nitrogen waste production, raising BUN levels through increased urea generation. Limiting protein to 0.8-1.0 grams per kilogram body weight reduces kidney workload.
Sodium restriction below 2,300 mg daily improves kidney function by reducing fluid retention and blood pressure. Plant-based proteins produce less nitrogen waste than animal proteins. Foods supporting kidney health include berries, leafy greens, whole grains, and omega-3 rich fish.
Avoiding processed meats, excess dairy, and high-phosphorus foods protects kidney function. Balanced nutrition with adequate calories prevents muscle breakdown that elevates BUN.
How Important Is Hydration in Reducing High BUN?
Hydration is essential in reducing high BUN because adequate fluid intake directly improves kidney filtration and urea excretion. Oral rehydration proves non-inferior to IV hydration in moderate chronic kidney disease patients. Pre-procedure hydration with 0.9% sodium chloride at 3 mL/kg/hour for one hour reduces contrast-induced acute kidney injury risk.
Continuing hydration 6-8 hours post-procedure prevents acute kidney injury development. Medical protocols recommend at least 500 cc fluid within 3 hours prior to contrast procedures. Daily water intake of 2-3 liters maintains optimal kidney function in healthy adults.
Dehydration concentrates BUN by reducing kidney perfusion and filtration capacity. The relationship between hydration and BUN levels determines treatment approaches for elevated values.
Are There Long-Term Strategies for Keeping BUN Within a Healthy Range?
Long-term strategies for keeping BUN within a healthy range include protocol-based monitoring, staged fluid management, and regular nephrology follow-up. Protocol-based strategies benefit high-risk patients including postoperative and septic shock cases. Four stages of IV fluid therapy encompass resuscitation, replacement, maintenance, and redistribution phases.
Nephrology consultation becomes necessary when eGFR drops below 60 mL/min/1.73m² at follow-up visits. Integration of acute kidney injury clinical decision support tools into electronic medical records shows statistically significant improved outcomes. Regular monitoring includes quarterly BUN checks for at-risk patients.
Exercise improves kidney perfusion through enhanced cardiovascular health. Weight management reduces kidney stress from metabolic demands. These integrated approaches maintain BUN levels within the normal 8-20 mg/dL range while preventing kidney disease progression.
How Can IV Fluid Therapy from The Drip IV Infusion Help With High BUN Levels?
IV fluid therapy from The Drip IV Infusion addresses high BUN levels through targeted hydration protocols that restore kidney function. Elevated BUN levels above 20 mg/dL signal dehydration or kidney stress requiring medical intervention. The Drip IV Infusion provides crystalloid solutions that increase renal blood flow and glomerular filtration rate. According to AAFP guidelines, isotonic crystalloids serve as first-line therapy for prerenal azotemia. Professional IV administration ensures proper fluid balance while monitoring for complications such as fluid overload or electrolyte imbalances.
What IV Fluid Options Does The Drip IV Infusion Offer for High BUN?
The Drip IV Infusion offers balanced crystalloid solutions specifically formulated for kidney support and BUN reduction. Normal saline (0.9% NaCl) containing 154 mEq/L sodium provides basic hydration for mild elevations. Lactated Ringer’s solution delivers superior kidney protection through balanced electrolytes that minimize chloride exposure. A 2018 clinical trial at Vanderbilt University on balanced crystalloids found 1.1% absolute risk reduction in composite renal outcomes compared to normal saline. The Drip IV Infusion administers bolus infusions of 10-20 mL/kg following NICE guidelines for optimal kidney perfusion. Specialized protocols include pre-procedure hydration at 3 mL/kg/hr for contrast exposure prevention. Each treatment plan incorporates monitoring parameters including urine output targets above 30 mL/hr and serial BUN measurements.
What Are the Key Takeaways About IV Fluids for High BUN Levels from This Guide?
The key takeaways about IV fluids for high BUN levels are that normal BUN range is 8-20 mg/dL with elevations indicating potential kidney dysfunction requiring prompt assessment. Balanced crystalloids demonstrate superior outcomes compared to normal saline for kidney protection through reduced chloride burden. Early fluid resuscitation within appropriate protocols can reverse prerenal azotemia within 24 hours in dehydration cases. Monitoring protocols include urine output >30 mL/hr, serial BUN/creatinine measurements every 6-12 hours, and volume status assessment through weight and vital signs. Contraindications encompass heart failure, existing fluid overload, and pulmonary edema risk requiring alternative management strategies. The Drip IV Infusion provides professional IV therapy services with medical oversight ensuring safe, effective BUN reduction through evidence-based hydration protocols tailored to individual kidney function needs.