If you’re concerned about potential complications from IV therapy, you’re not alone. Many patients and healthcare providers share these worries, especially given that infiltration affects up to 34% of patients in some settings and catheter-related infections can occur in nearly 40% of cases. We’re here to provide you with comprehensive, evidence-based information about IV therapy complications, their prevention, and treatment options to help you make informed decisions about your care.
Intravenous (IV) therapy complications are adverse events that occur during or after the administration of fluids, medications, or nutrients through a vein, ranging from minor infiltration affecting 1-34% of patients to serious bloodstream infections with rates of 0.8 per 1,000 catheter-days. These complications include infiltration/extravasation, phlebitis, catheter-related infections, air embolism, and fluid overload. Understanding these risks and implementing proper prevention strategies can reduce complication rates by up to 90% with modern monitoring technologies and evidence-based protocols.
TL;DR Summary
Our comprehensive guide covers the essential aspects of IV therapy complications in the order you’ll find detailed in this article:
• Common Complications – Infiltration occurs in 16.93% of pediatric surgery patients and phlebitis affects 20-30% of IV therapy recipients, while catheter-related bloodstream infections cost $3,000-$56,000 per episode to treat
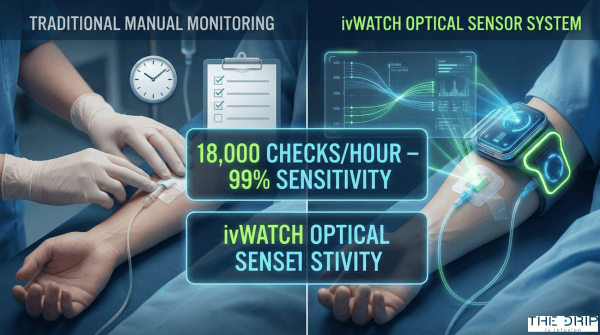
• Early Detection Methods – Continuous monitoring systems like ivWatch perform over 18,000 checks per hour and can detect infiltration at volumes as low as 0.2 mL with 99% sensitivity
• Prevention Strategies – Ultrasound-guided insertion increases first-attempt success from 32.5% to 85.7% in pediatric patients, while proper hand hygiene and aseptic technique remain fundamental
• Management Protocols – Immediate discontinuation, standardized treatment algorithms, and interdisciplinary teams reduce hospitalization rates from 50% to 0% for extravasation events
• At-Risk Populations – Neonates experience complication rates up to 80%, while elderly patients face increased risks due to fragile veins and fluid overload vulnerability
• Documentation Requirements – Joint Commission considers extravasation injuries sentinel events, requiring comprehensive documentation including drug/fluid type, catheter details, and patient outcomes
• Special Population Considerations – Pediatric S.T.I.C.K. bundle achieved 50% reduction in infiltration rates, while chlorhexidine is contraindicated in premature neonates
• Technology Advances – Smart infusion pumps with EHR integration and optical sensor monitoring have achieved 100% prevention of IV leakage incidents at some facilities
Quick Tip: Always ensure your IV site is checked at least daily through palpation and visual inspection – early detection of complications can prevent 90% of serious infiltration injuries when combined with prompt intervention.
Understanding these complications empowers you to actively participate in your care and recognize warning signs early. As we explore each aspect in detail, you’ll gain the knowledge needed to ensure safer IV therapy experiences.
What Are the Most Frequent Types of IV Therapy Complications?
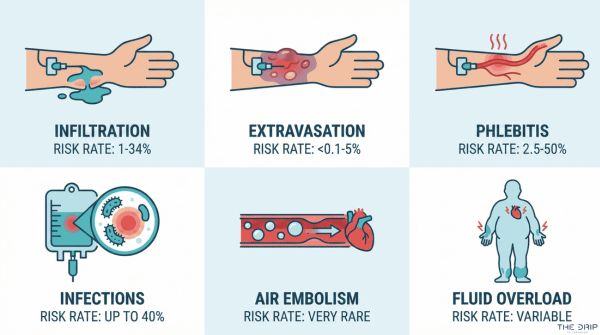
The most frequent types of IV therapy complications are infiltration, extravasation, phlebitis, infections, air embolism, and fluid overload. A Thai hospital study documented infiltration rates of 1.01% and extravasation rates of 0.60% across all IV sites. Phlebitis occurs in 20-30% of patients depending on population and catheter dwell time. These complications range from minor tissue irritation to life-threatening bloodstream infections affecting thousands of patients annually.
How Can Infiltration and Extravasation Occur During IV Therapy?
Infiltration and extravasation occur when IV fluids leak into surrounding tissues instead of entering the vein. Pediatric surgery patients experience a 16.93% incidence of peripheral intravenous infiltration and extravasation according to a study of 19,771 cases. Pediatric NICU populations show even higher rates at 34% incidence.
The upper extremity is involved in 89.6% of infiltration events, with a mean patient age of 36.7 years. Between August 2023 and January 2024, ivWatch monitoring detected 122 cases of infiltration/extravasation out of 2,254 infusions, representing a 5.4% detection rate.
Complications from infiltration include:
- Superficial soft tissue infection (8.6% of cases)
- Necrosis or eschar formation (3.2% of cases)
- Ulceration or full-thickness wounds (1.9% of cases)
- Long-term sequelae (5.1% of cases)
The INS Vesicant Task Force identified midline catheters as a possible risk factor for extravasation requiring thorough risk assessment. Recent cohort studies found no cases of compartment syndrome or fasciotomy required despite these complication rates.
What Causes Phlebitis and Thrombophlebitis in IV Therapy Patients?
Phlebitis and thrombophlebitis in IV therapy patients are caused by mechanical irritation, chemical irritation, or bacterial contamination of the catheter site. A Thai hospital reported a 2.41% phlebitis rate for level 1-2 severity. Peripheral IV catheters show a 1.25% incidence, increasing to 1.38% post-infusion.
Catheter dwell time beyond 72-96 hours significantly increases infection and phlebitis risk. The INS sets an acceptable thrombophlebitis incidence threshold at 5%. IV therapy teams demonstrate substantial impact, reducing cellulitis and suppurative phlebitis rates tenfold from 2.1% to 0.2%.
Which Infections Are Associated With IV Therapy?
The infections associated with IV therapy are catheter-related bloodstream infections (CRBSI), central line-associated bloodstream infections (CLABSI), and local site infections. Peripheral IV catheter-associated infection rates are 0.150% with an incidence of 65.1 per 100,000 catheter-days according to a 95% confidence interval study.
| Infection Type | Rate | Setting |
| CRBSI prevalence | 39.25% | Some populations |
| Hospital CRBSI | 1.99-4.05 per 1000 admissions | 2020-2023 data |
| Pediatric CLABSI | 4.49 per 1000 catheter-days | Central lines |
| Ambulatory CLABSI | 0.97 per 1000 central-line days | Outpatient settings |
| PICC infection | 3% (CLABSI: 1.4-1.9%) | 95% CI 3-4% |
| Median USA CLABSI | 0.8 per 1000 central line-days | 10% decrease 2023-2024 |
An estimated 18,100 CLABSIs occur annually in US hospitals, representing a significant healthcare burden.
What Are Air Embolism and Fluid Overload in the Context of IV Therapy?
Air embolism and fluid overload in IV therapy context are serious complications affecting cardiovascular and respiratory systems. Air embolism incidence ranges from 1 in 47 to 1 in 3,000 with IV catheter insertion or removal. Central venous catheter placement shows 0.1-1% air embolism incidence, while interventional radiology procedures have a 0.13% rate.
Fluid overload affects 1 in 5 hospitalized patients, though often underreported. Elderly, critically ill, and renal failure patients are particularly vulnerable to fluid overload complications. These conditions may cause respiratory distress, cardiovascular strain, and electrolyte imbalances requiring immediate medical intervention.
Understanding these complication rates helps healthcare providers implement targeted prevention strategies and monitoring protocols for safer IV therapy administration.
How Can Complications of IV Therapy Be Detected Early?
Complications of IV therapy can be detected early through systematic monitoring protocols and patient education. A 2024 ivWatch study of 2,254 infusions found optical sensor technology detected infiltration at volumes as low as 0.2 mL with 99% sensitivity for volumes greater than 10 mL. Early detection prevents severe tissue damage and reduces treatment costs. The following monitoring approaches and educational strategies help identify complications before they progress to serious adverse events.
What Signs and Symptoms Should Be Monitored During IV Therapy?
The signs and symptoms that should be monitored during IV therapy include erythema, warmth, tenderness at the insertion site, palpable venous cord, swelling, induration, and purulent drainage. CDC guidelines recommend daily palpation through the dressing and visual inspection when transparent dressings are used. Phlebitis severity ranges from Level 1 (erythema only) to Level 4 (erythema with edema, palpable cord, and fever).
Advanced monitoring systems enhance early detection capabilities. The ivWatch system performs over 18,000 checks per hour for infiltration and extravasation signs. A neonatal study of 32,713 insertions demonstrated a 90% reduction in the most serious infiltration grades with continuous optical monitoring.
Patient-reported complications occur in over 60% of cases after PICC placement, making patient feedback essential for early detection. Healthcare providers should assess insertion sites at each interaction and document any changes in appearance or patient-reported discomfort. Regular monitoring combined with technology-assisted detection creates multiple safety checkpoints throughout IV therapy administration.
How Does Patient Education Help Identify IV Therapy Complications?
Patient education helps identify IV therapy complications by empowering patients to recognize early warning signs and report symptoms promptly. The 2024 WHO guidelines specifically include patients as an intended audience for IV therapy protocols, acknowledging their critical role in complication detection. Parent involvement in pediatric IV care demonstrated improved outcomes in S.T.I.C.K. bundle implementation studies.
Educated patients can identify subtle changes such as burning sensations, coolness around the insertion site, or restricted movement that may indicate developing complications. Teaching patients to monitor for redness, swelling, or discharge enables earlier intervention before complications progress. This collaborative approach between healthcare providers and patients strengthens the safety monitoring network and reduces the severity of complications when they occur.
What Preventive Measures Reduce the Risk of IV Therapy Complications?
Preventive measures reduce the risk of IV therapy complications through proper insertion techniques, sterile equipment protocols, and continuous site monitoring. The following evidence-based strategies demonstrate significant reductions in infiltration, infection, and phlebitis rates.
How Do Proper Insertion Techniques and Site Selection Prevent Complications?
Proper insertion techniques and site selection prevent complications by increasing first-attempt success rates and reducing mechanical trauma. Ultrasound-guided insertion achieves 85.7% first-attempt success compared to 32.5% for standard technique in pediatric patients according to clinical trials. Adults with difficult venous access show 63.9% success with ultrasound versus 13.9% with standard techniques. A meta-analysis demonstrates a 2-fold increase in first-pass success with ultrasound guidance.
Site selection follows CDC Category IA guidelines prioritizing upper extremity placement for adults. Lower extremity catheters require immediate replacement when alternative sites become available. The subclavian vein is preferred over jugular or femoral sites for central venous catheters per CDC Category IB recommendations. Areas of flexion should be avoided due to increased risks of phlebitis, infiltration, and catheter dislodgment according to INS standards.
Ultrasound guidance prevented central venous catheter placement in 85% of patients with difficult IV access. These techniques reduce multiple insertion attempts that damage vessel walls and increase complication risks.
Why Is Equipment Sterility and Hand Hygiene Critical for Prevention?
Equipment sterility and hand hygiene are critical for prevention because they eliminate pathogen transmission during catheter insertion and maintenance. CDC Category IA guidelines mandate hand hygiene and aseptic technique as fundamental prevention measures. Maximal sterile barrier precautions during central line insertion include sterile gloves, gowns, masks, and full-body drapes.
Chlorhexidine skin antisepsis significantly reduces infection rates compared to povidone-iodine preparations. A systematic review identified wearing gloves during insertion as an effective prevention measure. Using the minimum number of ports and lumens reduces infection risk per CDC Category IB recommendations.
Central line bundles incorporating sterility measures achieved 56% CLABSI reduction across 59 studies. These protocols demonstrate consistent infection prevention when implemented systematically.
How Important Is Site Monitoring and Care in Preventing IV Complications?
Site monitoring and care are essential in preventing IV complications through early detection and proper maintenance protocols. CDC Category IB guidelines require daily insertion site monitoring by palpation and inspection. Gauze dressings require replacement every 2 days, while transparent dressings need changing at least every 7 days.
Chlorhexidine-impregnated dressings are recommended for adults over 18 years per CDC Category IA guidelines but contraindicated for premature neonates. Peripheral catheters do not require routine replacement more frequently than every 72-96 hours for infection prevention. Prompt catheter removal when no longer essential prevents unnecessary complication risks.
Emergency-inserted catheters require replacement within 48 hours per CDC Category IB recommendations. Frimley Health NHS achieved 100% prevention of IV leakage incidents using continuous monitoring systems. These monitoring protocols enable intervention before complications develop into serious adverse events.
How Should IV Therapy Complications Be Managed and Treated?
IV therapy complications require immediate recognition and systematic management protocols to prevent serious outcomes. Management approaches vary based on complication type, severity, and patient factors. Early intervention reduces hospitalization rates from 50% to near zero with proper protocols.
What Are the Immediate Steps to Take If a Complication Occurs?
The immediate steps to take if a complication occurs are stopping the infusion, assessing the site, documenting findings, and initiating specific interventions based on complication type. Chemotherapy extravasation managed by interdisciplinary task forces shows satisfactory outcomes with standardized protocols. Dexrazoxane administration reduces tissue necrosis requiring surgical intervention in chemotherapy extravasation cases.
Key immediate actions include:
- Stop infusion immediately upon detecting complications
- Leave catheter in place for severe extravasations to aspirate residual drug
- Apply cold or warm compresses based on drug type
- Elevate affected limb to reduce swelling
- Mark infiltration borders with permanent marker
- Photograph the site for documentation
- Notify physician and pharmacy immediately
A 479-patient study found six infiltrations required debridement with or without grafting. Hospitalization rates for extravasation range from 0-50% depending on management approach timing and protocol adherence. Rapid response teams specializing in IV complications reduce severe outcomes through immediate assessment and intervention.
When Should IV Infusion Be Discontinued Due to a Complication?
IV infusion should be discontinued when signs of phlebitis, infection, infiltration, or catheter malfunction appear. INS standards require removing catheters if phlebitis, infection, or malfunction signs develop. Opaque dressings must be removed if patients have tenderness or infection signs for proper assessment.
Discontinuation criteria include:
- Phlebitis grade 2 or higher (erythema with pain or edema)
- Purulent drainage at insertion site
- Infiltration with coolness, swelling, or decreased flow rate
- Patient reports burning, stinging, or severe discomfort
- Fever of unknown origin with catheter in place >48 hours
- Positive blood culture suggesting catheter-related infection
Daily evaluation of insertion sites guides removal decisions. Catheters inserted during emergencies require replacement within 48 hours due to higher contamination risk. Documentation of removal reasons supports quality improvement efforts and regulatory compliance.
What Medical Interventions Are Available for Specific IV Complications?
Medical interventions for specific IV complications range from topical treatments to surgical debridement, with costs varying significantly by severity. CRBSI treatment costs range from $3,000 to $56,000 per episode. CLABSI treatment prolongs hospital admission by 7-14 days on average.
| Complication Type | Intervention | Cost Impact | Outcome |
| CRBSI | Systemic antibiotics | $3,000-$56,000 | 7-14 day hospital extension |
| CLABSI (PICC) | Antimicrobial therapy | ¥87,147.08 per patient | Reduced with coated catheters |
| Severe infiltration | Surgical debridement | Tens of thousands (UK) | Variable recovery time |
| Extravasation | Dexrazoxane | Variable | Reduced tissue necrosis |
Antimicrobial-coated PICCs reduce CLABSI cases significantly, showing 0 infections versus 3 in standard groups. Severe infiltration and extravasation treatments in the UK cost tens of thousands of pounds per case. Early intervention with appropriate antidotes may prevent surgical intervention needs. Treatment selection depends on infiltrated substance, volume, location, and time since occurrence.
Understanding proper management protocols ensures rapid response to IV therapy complications. The next section examines which patients face highest complication risks and why certain populations require special monitoring approaches.
Who Is Most at Risk for IV Therapy Complications and Why?
Certain patient populations face significantly higher risks of IV therapy complications due to physiological factors and underlying health conditions. Understanding these risk factors helps healthcare providers implement targeted prevention strategies and monitoring protocols for vulnerable groups.
What Patient Factors Increase the Risk of Complications?
Patient factors that increase complication risk include age, body mass index, catheter characteristics, and medication types. A pediatric study identified sex, age, disease classification, puncture site, and indwelling time as significant risk factors for complications. IV crystalloids administration increases complication risk (P= 0.03), while IV analgesic drugs show even stronger association (P=.001).
Age is statistically significant for extravasation risk (P=.001). Adult patients with higher BMI, diabetes mellitus, chronic renal failure, and malignancy experience increased PICC complications. Multiple lumen catheters correlate with higher complication rates compared to single lumen devices.
Catheter dwell time directly impacts risk levels. Longer indwelling periods are associated with increased mechanical failures and infections. Advanced age emerges as a consistent risk factor for both PICC and midline catheter complications across multiple studies.
How Do Underlying Health Conditions Affect Complication Risk?
Underlying health conditions affect complication risk through altered physiology and compromised immune function. CHF patients with peripheral IV complications experience doubled length of hospital stay, doubled ICU admission rates, and five times higher mortality risk compared to those without complications.
Neonates demonstrate complication rates up to 80% due to fragile vessels and immature systems. Immunocompromised patients face susceptibility to bacterial, fungal, viral, and parasitic infections beyond typical bacterial risks.
Renal failure patients are particularly vulnerable to fluid overload and electrolyte imbalances due to impaired kidney function. Cancer patients experience higher mechanical failure rates with PICCs. PICC-related venous thrombosis occurs in 6.7-10.6% of symptomatic cancer patients, requiring anticoagulation management.
These high-risk populations require enhanced monitoring protocols, specialized insertion techniques, and careful device selection to minimize complications while maintaining necessary vascular access for treatment.
How Should Complications of IV Therapy Be Documented and Reported?
Accurate documentation of IV therapy complications is essential for patient safety and regulatory compliance. Complete patient medical records must include full accounts of adverse events with drug/fluid involved, VAD type, and stage/severity. The FDA MAUDE database requires mandatory reporting from manufacturers, importers, and device user facilities. Documentation enables tracking of 28 million+ spontaneous reports in the FDA FAERS system. Patient harm, injury, complication, or negative outcome documentation ensures legal compliance. These comprehensive records protect both patients and healthcare providers while contributing to improved IV therapy safety standards.
Why Is Accurate Documentation Important in IV Therapy?
Accurate documentation in IV therapy is critically important for patient safety, legal compliance, and quality improvement. Complete patient medical records must contain full accounts of any adverse event including the specific drug or fluid involved, VAD type, and stage/severity classification. The FDA maintains the MAUDE database which mandates reporting from manufacturers, importers, and device user facilities whenever complications occur. According to FDA data, documentation systems enable tracking of over 28 million spontaneous reports in the FAERS system, providing invaluable safety surveillance. Healthcare facilities face legal requirements to document all instances of patient harm, injury, complication, or negative outcomes related to IV therapy. This documentation serves multiple purposes such as protecting patient rights, supporting healthcare providers in legal matters, and contributing to national safety databases that identify trends and improve protocols.
What Are Best Practices for Reporting IV Therapy Complications?
Best practices for reporting IV therapy complications include following standardized protocols from regulatory agencies and professional organizations. The Joint Commission classifies extravasation injuries as sentinel events, with approximately 800 cases reported annually since 2007. CDC NHSN requires facilities to submit monthly CLABSI data within 30 days of each month’s end for national surveillance. Healthcare providers must complete FDA Form 3500 for adverse event reporting, including detailed clinical information about the incident. HIPAA compliance remains mandatory for all IV therapy information documentation to protect patient privacy. State health departments require additional reporting for validation purposes in their jurisdictions. Unanticipated problems involving risks to patients must be reported promptly to relevant regulatory agencies including institutional review boards when research protocols are involved. These reporting requirements create a comprehensive safety network that identifies patterns, prevents future complications, and ensures accountability across the healthcare system.
How Is IV Therapy Complication Prevention and Management Different in Special Populations?
IV therapy complication prevention and management differs in special populations due to unique physiological characteristics and vulnerability factors. Pediatric patients demonstrate 34.0% to 56.0% overall complication prevalence, while elderly and immunocompromised populations require specialized protocols. These populations need modified insertion techniques, dosing adjustments, and enhanced monitoring strategies.
What Additional Considerations Are Needed for Pediatric and Geriatric Patients?
The additional considerations for pediatric and geriatric patients include age-specific complication rates, anatomical differences, and specialized prevention protocols. Neonatal NICU populations show 34% peripheral IV infiltration and extravasation (PIVIE) incidence, with rates reaching 80% in some populations. The CDC Category IC guideline specifically contraindicates chlorhexidine use in premature neonates due to skin sensitivity.
Pediatric considerations require specialized approaches:
- Smaller vessel size increases infiltration risk
- Higher metabolic rates affect fluid requirements
- Limited communication ability necessitates objective monitoring
- Parent involvement through protocols like S.T.I.C.K. bundle
A 2023 study implementing the pediatric S.T.I.C.K. bundle achieved 50% reduction in infiltration rates through structured parent involvement. This protocol engages caregivers in monitoring for early complication signs.
Geriatric patients present unique challenges due to age-related vascular changes. Elderly patients have fragile veins prone to bruising, with dehydration and tissue elasticity loss complicating venous access. These physiological changes increase risks for:
- Vessel trauma during insertion
- Infiltration from fragile vein walls
- Hematoma formation
- Delayed healing
Fluid management requires particular attention in geriatric populations. Older adults have increased fluid overload vulnerability due to decreased cardiac reserve and renal function. Careful monitoring prevents complications such as pulmonary edema and electrolyte imbalances.
Understanding these population-specific factors enables healthcare providers to implement targeted prevention strategies and improve IV therapy outcomes.
How Are Immunocompromised Patients Managed Differently Regarding IV Therapy Risks?
Immunocompromised patients are managed differently regarding IV therapy risks through enhanced aseptic precautions, specialized catheter selection, and intensive monitoring protocols. These patients have higher infection risk, requiring more aggressive prevention measures than standard populations.
Enhanced infection prevention includes:
- Maximal sterile barrier precautions during all procedures
- Antimicrobial-coated catheter consideration for high-risk cases
- Increased frequency of site assessment
- Lower threshold for catheter replacement
The immunocompromised population’s susceptibility extends to a broader range of pathogens. While standard patients primarily face bacterial risks, immunocompromised individuals may develop infections from bacteria, fungi, viruses, and parasites. This expanded pathogen spectrum necessitates:
- Comprehensive antimicrobial prophylaxis protocols
- Specialized laboratory monitoring
- Multidisciplinary care coordination
- Early intervention strategies
Catheter selection becomes critical in this population. Healthcare providers must consider antimicrobial-coated lines for high-risk immunocompromised patients, balancing infection prevention benefits against potential complications. The decision requires individual risk assessment considering factors such as expected therapy duration, neutropenia severity, and previous infection history.
Special populations require individualized IV therapy approaches that account for their unique vulnerabilities and complication risks, ensuring optimal outcomes while minimizing adverse events.
How Can Recent Advances and Innovations Reduce IV Therapy Complication Rates?
Recent advances and innovations reduce IV therapy complication rates through automated monitoring systems, ultrasound-guided placement technology, and evidence-based training protocols. The ivWatch system achieved 100% prevention of IV leakage incidents at Frimley Health NHS through continuous optical monitoring. Smart infusion pumps with EHR integration and drug libraries containing standardized dosing parameters prevent medication errors. These technological improvements combined with specialist training programs demonstrate measurable reductions in infiltration, infection, and medication administration complications.
What New Devices or Protocols Improve IV Therapy Safety?
New devices and protocols that improve IV therapy safety include real-time monitoring systems, advanced ultrasound guidance, and antimicrobial catheter materials. The ivWatch system prevented 100% of IV leakage incidents at Frimley Health NHS by performing over 18,000 checks per hour. BD launched the SiteRite 9 Ultrasound System in November 2023 for enhanced vessel assessment before insertion. Medtronic introduced an advanced IV infiltration detection system in March 2023.
Hydrophobic polyurethane PICC catheters demonstrate significantly lower complication rates at 21.5% compared to 38.6% for standard PICC lines. Smart infusion pumps with EHR integration reduce medication administration errors through automated verification. Drug libraries with guardrails technology prevent dosing errors by establishing safe administration parameters.
The IV Infiltration Detection Device Market reflects this technological advancement, growing from $331.9 million in 2023 to a projected $479.9 million by 2032. Automatic medication replacement devices currently in development for 2025 release will further enhance safety protocols.
How Do Technology and Training Impact Complication Reduction?
Technology and training impact complication reduction through specialized teams, certification programs, and quality improvement bundles. Vascular access specialist teams reduce catheter-related bloodstream infection incidence and overall complications significantly. According to a 2024 WHO report, registered nurses with ultrasound training achieve 95% first-stick success rates.
IV therapy certification requires 27-36 hours of training with competency verification. Quality improvement bundles containing 2-7 components show significant reductions in phlebitis and bloodstream infections. The S.T.I.C.K. bundle implementation demonstrated dramatic decreases in infiltrations 5-6 months post-implementation.
The 2024 WHO guidelines provide evidence-informed approaches for insertion, maintenance, access, and removal procedures. INS Standards updated in 2024 include 66 standards supported by over 2,500 references for evidence-based practice. The PVAM care bundle approach generates €2.11 savings per procedure with 3.51% annual savings, demonstrating both clinical and economic benefits of structured training programs.
How Can You Safely Experience IV Therapy With The Drip IV Infusion?
The Drip IV Infusion ensures safe IV therapy through rigorous medical protocols and professional supervision. The company employs licensed medical professionals who follow CDC guidelines for insertion, monitoring, and removal of IV catheters. Patient safety begins with comprehensive health screening before treatment to identify risk factors such as underlying conditions or medication interactions. The Drip IV Infusion maintains sterile environments and uses pharmaceutical-grade ingredients to minimize infection risks that affect 0.150% of peripheral IV catheter patients according to recent clinical data.
How Does The Drip IV Infusion Help Prevent and Address IV Therapy Complications?
The Drip IV Infusion prevents IV therapy complications through multiple safety layers including ultrasound-guided insertion, continuous monitoring, and immediate intervention protocols. Ultrasound guidance increases first-attempt success rates to 85.7% compared to 32.5% with standard techniques based on pediatric studies. The company’s trained professionals monitor for infiltration signs, which occur in 5.4% of infusions according to 2024 ivWatch data. Staff members follow aseptic techniques that reduced CLABSI rates by 56% in multi-site studies. The Drip IV Infusion maintains emergency protocols for managing complications such as extravasation or phlebitis, with immediate discontinuation and medical referral when indicated.
What Should You Remember About IV Therapy Complications, Prevention, and Treatment?
IV therapy complications carry significant health and economic impacts that proper prevention can minimize. A 2009 CDC analysis found that CLABSI prevention efforts prevented 25,000 infections, saved 6,000 lives, and avoided $414 million in excess healthcare costs. Prevention programs generated $5.7-$31.5 billion in direct medical cost savings according to CDC-sponsored research. The economic burden varies by device type: CVC complications cost $3,074.79, midline catheters $1,424.02, PICC lines $1,302.07, and peripheral venous catheters $328.33 per incident. First-attempt IV insertion costs $28-$35 while home infusion averages $122 daily versus $798 for inpatient care. IV therapy sessions range from $85-$400, making prevention both medically prudent and economically essential for patients seeking safe treatment options.