If you’re wondering whether IV or oral antibiotics are better for your infection, you’re asking a critical question that could significantly impact your recovery, comfort, and healthcare costs. We understand the uncertainty and concern that comes with making medical decisions, especially when traditional medical wisdom seems to conflict with emerging evidence. This comprehensive guide addresses your concerns with the latest 2026 research and clinical data to help you make an informed choice alongside your healthcare provider.
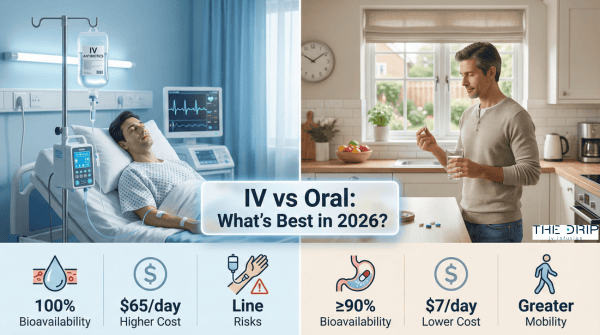
IV versus oral antibiotics represents a fundamental shift in how we approach infection treatment, challenging decades of medical dogma with compelling new evidence. The growing body of research from 2023-2026 demonstrates that for many stable patients, oral antibiotics with high bioavailability (≥90%) achieve therapeutic outcomes equivalent to or better than intravenous administration, while offering improved safety profiles, reduced healthcare costs, and enhanced quality of life—a paradigm shift that infectious disease experts now describe as “oral is the new IV.”
TL;DR Summary:
• IV antibiotics work by achieving 100% bioavailability through direct bloodstream delivery, traditionally reserved for serious infections, though recent evidence challenges the necessity of this approach for many conditions.
• Oral antibiotics with ≥90% bioavailability (including fluoroquinolones, linezolid, and metronidazole) can achieve serum concentrations comparable to IV administration while avoiding catheter-related complications.
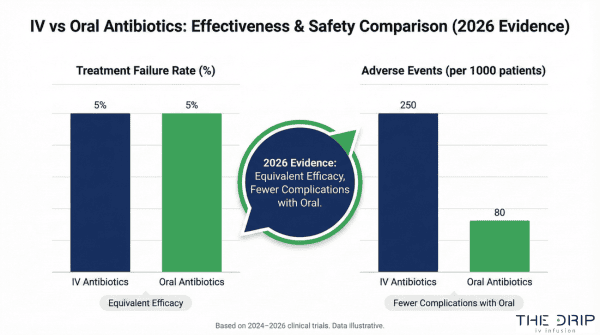
• Effectiveness comparison studies from 2025-2026 show no difference in treatment failure rates between oral and IV antibiotics for bone infections, bacteremia, and selected endocarditis cases, with oral therapy actually reducing mortality in gram-negative bacteremia.
• Practical considerations favor oral antibiotics with 9-fold lower daily costs ($7 vs $65), 4-day shorter hospital stays, and significantly improved patient mobility and quality of life.
• Overuse risks and resistance concerns make IV-to-oral switch programs a CDC-recommended core element of antimicrobial stewardship, with interventions reducing overall antibiotic use by up to 32%.
• Decision-making should prioritize patient stability, infection severity, and oral antibiotic bioavailability (≥70% minimum), with patients encouraged to ask about early switch opportunities.
• The Drip IV Infusion and emerging technologies leverage AI-driven approaches and nanotechnology to optimize antibiotic selection and delivery, supporting personalized treatment decisions in 2026.
Quick Tip: When discussing antibiotic options with your provider, always ask about the bioavailability percentage of any proposed oral antibiotic—if it’s above 90%, you’re likely getting the same therapeutic benefit as IV administration without the associated risks and inconvenience of catheter placement.
The evidence overwhelmingly supports a fundamental reconsideration of how we approach antibiotic administration, moving away from the reflexive use of IV therapy toward a more nuanced, patient-centered approach that recognizes oral antibiotics as the preferred option for many infections when clinically appropriate.
What Are IV Antibiotics and How Do They Work?
IV antibiotics are medications delivered directly into the bloodstream through a vein. These drugs achieve 100% bioavailability by bypassing the gastrointestinal absorption process. Intravenous administration has been the traditional standard for serious infections based on decades of clinical practice, though evidence now challenges this approach. The following subsections explore administration methods, suitable infections, advantages, and potential risks of IV antibiotic therapy.
How Are IV Antibiotics Administered?
IV antibiotics are administered through catheter insertion into a peripheral or central vein. This process requires skilled nursing care and sterile technique. According to a 2024 cost analysis study, administration costs for outpatient parenteral antibiotic therapy (OPAT) average $65 per day compared to $7 per day for oral therapy. IV administration carries risks of line-related complications, such as catheter-related bloodstream infections, thrombophlebitis, and deep vein thrombosis. Peripheral IV catheters typically require replacement every 72-96 hours to minimize infection risk.
What Types of Infections Are Commonly Treated with IV Antibiotics?
The types of infections commonly treated with IV antibiotics are bacteremia, osteomyelitis, endocarditis, and other serious systemic infections. Healthcare providers have traditionally preferred IV therapy for these conditions based on historical practice patterns. A 2022 systematic review of 21 prospective controlled trials found no studies showing superior efficacy for IV-only therapy compared to oral step-down for these conditions. Severe pneumonia, meningitis, and sepsis may still require initial IV treatment. The choice depends on infection severity, pathogen susceptibility, and patient stability.
What Are the Main Advantages of IV Antibiotics?
The main advantages of IV antibiotics are guaranteed 100% drug bioavailability and immediate systemic circulation. This route ensures predictable drug levels regardless of gastrointestinal function. IV antibiotics may be necessary for patients unable to take oral medications due to vomiting, unconsciousness, or nil-by-mouth status. Patients with severe gastrointestinal malabsorption disorders benefit from IV administration. Critical illness with hemodynamic instability may require IV therapy for rapid therapeutic levels.
What Are the Potential Risks or Side Effects of IV Antibiotics?
The potential risks of IV antibiotics are line-related complications and increased adverse events. The COPAT trial (2026) found IV-only therapy had more than double the rate of adverse events compared to early oral transition. Line-related complications include:
- Infiltration and extravasation causing tissue damage
- Catheter malfunction requiring replacement
- Phlebitis at insertion sites
- Air embolism from improper administration
IV administration does not significantly reduce antibiotic-associated diarrhea or Clostridioides difficile infection rates compared to oral therapy for most broad-spectrum agents. These gastrointestinal complications occur regardless of administration route.
What Are Oral Antibiotics and How Do They Function?
Oral antibiotics are antimicrobial medications taken by mouth that achieve therapeutic blood levels through gastrointestinal absorption. Fluoroquinolones such as levofloxacin and moxifloxacin achieve bioavailability of 90% or higher. Linezolid, metronidazole, clindamycin, trimethoprim-sulfamethoxazole, and doxycycline also demonstrate excellent oral bioavailability exceeding 90%. These high-bioavailability oral antibiotics can achieve serum concentrations comparable to intravenous administration. The following sections examine absorption mechanisms, suitable conditions, benefits, and limitations of oral antibiotic therapy.
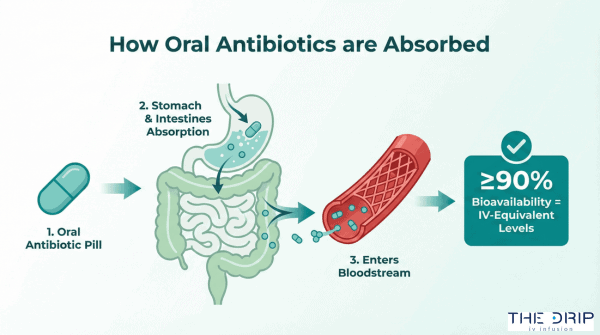
How Are Oral Antibiotics Taken and Absorbed?
Oral antibiotics are taken as tablets, capsules, or liquid formulations that require gastrointestinal absorption to reach systemic circulation. Bioavailability ranges from less than 40% for most cephalosporins and beta-lactams to 90% or higher for fluoroquinolones and linezolid. Experts recommend selecting oral antibiotics with at least 70% bioavailability for serious infections. Antibiotics with bioavailability exceeding 90% enable seamless IV-to-oral transitions. The absorption process depends on factors such as gastric pH, intestinal motility, and drug formulation.
What Conditions Are Most Suitable for Oral Antibiotics?
The conditions most suitable for oral antibiotics include pyelonephritis, cellulitis, bone and joint infections, gram-negative bacteremia, and selected endocarditis cases. A 7-day course of oral ciprofloxacin provides safe and successful treatment for pyelonephritis. Oral therapy for cellulitis reduces hospital admission by 2.6 days compared to IV therapy. Stable patients with bone and joint infections respond equally well to oral antibiotics as IV treatment. Gram-negative bacteremia and certain infective endocarditis cases show equivalent outcomes with oral therapy.
What Benefits Do Oral Antibiotics Offer?
The benefits of oral antibiotics are convenience, independence, earlier hospital discharge, and quicker return to normal activities. Patients prefer oral antibiotics because they eliminate the need for IV catheters and allow greater mobility. Oral therapy reduces nursing workload and healthcare resource utilization compared to IV administration. Freedom from IV lines significantly improves patient quality of life. The cost savings from oral therapy average $58 per day compared to outpatient parenteral therapy.
What Limitations or Side Effects Come with Oral Antibiotics?
The limitations of oral antibiotics include poor bioavailability for certain drug classes and gastrointestinal side effects. Most cephalosporins and beta-lactams have bioavailability below 40%, making them unsuitable for serious systemic infections. Gastrointestinal side effects such as diarrhea represent the primary adverse events with oral antibiotics. Azithromycin and ciprofloxacin demonstrate moderate bioavailability between 40-90% and may require dose adjustments. Patients with severe nausea, vomiting, or malabsorption disorders may not tolerate oral antibiotics effectively. Understanding these limitations helps clinicians select appropriate candidates for oral antibiotic therapy while optimizing treatment outcomes.
How Do IV and Oral Antibiotics Compare in Terms of Effectiveness?
IV and oral antibiotics compare in terms of effectiveness with no significant difference in treatment outcomes for most serious infections when appropriate oral agents are selected. A 2025 meta-analysis of 9 randomized controlled trials found no difference in treatment failure rates between oral and IV antibiotics for bone and joint infections. Early switch to oral therapy for gram-negative bacteremia was associated with lower mortality (6.9% vs 14.3%) compared to prolonged IV treatment in a 2024 study. The following sections examine specific scenarios where one route may offer advantages over the other.
In Which Situations Are IV Antibiotics More Effective Than Oral?
IV antibiotics are more effective than oral in patients who cannot tolerate oral medications or have severe malabsorption disorders. In a 2025 study of emergency department-discharged community-acquired pneumonia patients, IV antibiotics showed lower 30-day revisit rates, though the IV group had more severe initial presentations. IV therapy remains necessary for critically unstable patients and those with documented gastrointestinal absorption issues.
When Is Oral Therapy Sufficiently Effective?
Oral therapy is sufficiently effective for most clinically stable patients with infections caused by susceptible organisms. The Therapeutics Letter (May 2025) recommends oral antibiotics as standard of care for most stable patients. Switching to partial oral treatment is as effective as traditional 4-6 weeks of IV therapy for selected infective endocarditis patients. High-bioavailability oral antibiotics achieve therapeutic concentrations comparable to IV administration.
Are There Conditions Where Both Methods Are Equally Effective?
There are conditions where both methods are equally effective, including osteomyelitis, bacteremia, and endocarditis in stable patients. According to 21 prospective controlled trials, oral step-down therapy was at least as effective as IV-only for these serious infections. For clinically stable patients with infections caused by organisms susceptible to high-bioavailability oral antibiotics, both routes show equivalent outcomes. The key determinant is selecting oral antibiotics with bioavailability exceeding 70%.
What Does the Latest Research Say About IV vs Oral Antibiotics in 2026?
The latest research about IV vs oral antibiotics in 2026 demonstrates superior safety profiles for oral therapy. The COPAT trial (January 2026) demonstrated early IV-to-oral transition resulted in two-fold reduction in total adverse events compared to IV-only therapy. Dr. Brad Spellberg’s 2022 systematic review concluded oral antibiotics are at least as effective, safer, and lead to shorter hospitalizations than IV-only therapy. These findings challenge decades of clinical practice favoring IV administration for serious infections.
What Are the Practical Considerations When Choosing Between IV and Oral Antibiotics?
The practical considerations when choosing between IV and oral antibiotics include cost differences, hospital stay length, and patient factors. Drug acquisition and administration costs show a 9-fold difference between outpatient parenteral antibiotic therapy (OPAT) at $65 per day and oral therapy at $7 per day. Early IV-to-oral switch reduces hospital length of stay by up to 4 days. Patient tolerance, lifestyle needs, and clinical guidelines shape the final treatment decision.
How Do Patient Factors Influence the Choice of Antibiotic Route?
Patient factors influencing antibiotic route choice include medication tolerance, gastrointestinal function, and treatment preferences. A 2025 patient perception study reveals that while many patients initially believe IV antibiotics are more effective, the majority prefer oral routes for convenience and independence. The patient’s ability to tolerate oral medications determines route feasibility. Gastrointestinal absorption issues may necessitate IV administration. Healthcare providers must balance clinical needs with patient preferences when selecting the optimal delivery method.
What Role Do Cost and Accessibility Play in the Decision?
Cost and accessibility play decisive roles through drug expenses, hospital resources, and healthcare system savings. Oral antibiotics offer substantial economic benefits including reduced drug costs, shorter hospital stays, and lower resource utilization. The 9-fold cost difference between OPAT and oral therapy creates significant budget implications for healthcare systems. Antimicrobial stewardship programs promoting IV-to-oral switch demonstrate measurable healthcare cost savings. Resource availability and insurance coverage may influence route selection in different healthcare settings.
Are There Legal or Medical Guidelines Shaping This Choice in 2026?
Legal and medical guidelines shaping antibiotic route choice in 2026 include CDC recommendations and updated clinical protocols. The CDC recommends automatic IV-to-oral switch programs as a core element of hospital antibiotic stewardship. Recent clinical guidelines increasingly support oral antibiotics as standard care for stable patients with appropriate drug selection. Healthcare facilities implement evidence-based protocols for early transition from IV to oral therapy. These guidelines reflect growing evidence supporting oral antibiotic efficacy for serious infections.
How Does Patient Lifestyle Affect IV vs Oral Selection?
Patient lifestyle affects IV versus oral selection through mobility needs, work schedules, and quality of life considerations. Oral therapy allows earlier hospital discharge and faster return to normal activities. Patients on oral antibiotics maintain greater mobility and independence compared to those requiring IV access. Work obligations and family responsibilities favor oral administration when clinically appropriate. The freedom from IV lines and medical appointments significantly improves daily functioning and treatment adherence.
What Are the Potential Risks of Overusing IV or Oral Antibiotics?
The potential risks of overusing IV or oral antibiotics include antimicrobial resistance development and increased adverse events. Overuse of IV antibiotics drives antimicrobial resistance emergence. A 2025 systematic review found antimicrobial stewardship interventions reduced overall antibiotic use by up to 32%. Both administration routes contribute to resistance when used inappropriately. The following subsections explore resistance impacts, adverse reactions, and risk minimization strategies.
How Does Antibiotic Resistance Impact the Selection of Administration Route?
Antibiotic resistance impacts the selection of administration routes by favoring oral therapy to reduce overall exposure. IV-to-oral switch programs slow resistant pathogen emergence by reducing IV therapy duration and total antibiotic exposure. Pharmacist-led interventions promote safe conversion from IV to oral therapy. These programs decrease selection pressure for resistance while maintaining treatment efficacy. Early oral transition reduces healthcare-associated infection risks that contribute to resistance spread.
What Are the Risks of Adverse Reactions or Complications for Each Method?
The risks of adverse reactions for each method differ in type but not severity. IV therapy complications include catheter-related bloodstream infections, thrombophlebitis, infiltration, and extravasation. Oral antibiotics primarily cause gastrointestinal side effects such as nausea, diarrhea, and abdominal discomfort. Both routes show similar rates of C. difficile infection for broad-spectrum agents. IV administration carries additional mechanical risks from catheter placement and maintenance.
How Can Patients Minimize Risks When Using Antibiotics?
Patients can minimize risks when using antibiotics through careful drug selection and monitoring. Selection of oral antibiotics with high bioavailability (≥90%) minimizes treatment failure risk while avoiding IV-related complications. Examples include linezolid, levofloxacin, and metronidazole. Therapeutic drug monitoring advances allow individualized antibiotic dosing to enhance safety and efficacy. Patients should complete prescribed courses and report adverse effects promptly. Understanding these risk reduction strategies helps optimize antibiotic therapy outcomes while limiting resistance development.
How Should You Decide Between IV and Oral Antibiotics?
The decision between IV and oral antibiotics requires evaluating patient stability, infection severity, pathogen susceptibility, and oral drug bioavailability. Recent evidence demonstrates oral antibiotics with bioavailability above 70% achieve therapeutic outcomes comparable to IV therapy for many serious infections. This section explores the key questions patients should ask, factors clinicians must consider, and the critical role of patient education in making informed treatment choices.
What Questions Should Patients Ask Their Provider When Choosing?
Patients should inquire about the bioavailability of proposed oral antibiotics and whether they exceed the 70% threshold recommended for serious infections. Bioavailability determines how much medication reaches systemic circulation—IV antibiotics achieve 100% bioavailability while oral options range from less than 40% to over 90%. Understanding expected therapy duration and potential for early IV-to-oral switch helps patients anticipate treatment timelines and recovery expectations.
Additional questions include asking about line-related complication risks versus gastrointestinal tolerance concerns. Patients should request specific data comparing outcomes for their infection type, as a 2022 systematic review of 21 prospective controlled trials found no studies showing superior efficacy for IV-only therapy compared to oral step-down for bacteremia, osteomyelitis, and endocarditis.
What Factors Should Clinicians Consider Before Recommending a Route?
Clinicians should evaluate patient stability, infection severity, pathogen susceptibility, and oral antibiotic bioavailability when selecting administration route. The evidence shows “oral is the new IV” for many infections, challenging decades of clinical dogma according to infectious disease experts. Key considerations include:
- Patient’s ability to tolerate oral medications
- Availability of high-bioavailability oral options (≥90% preferred)
- Infection site and organism susceptibility patterns
- Healthcare setting and monitoring capabilities
A 2026 COPAT trial demonstrated early IV-to-oral transition resulted in two-fold reduction in total adverse events compared to IV-only therapy. Cost differences averaging $65 per day for outpatient parenteral therapy versus $7 for oral therapy may influence decisions in resource-limited settings.
How Important Is Patient Education in the Decision-Making Process?
Patient education is crucial as many initially believe IV antibiotics are more effective despite evidence showing equivalent or superior outcomes with oral therapy. A 2025 patient perception study revealed this misconception persists even when presented with clinical data. Understanding the safety profile and convenience benefits of oral antibiotics helps patients make informed treatment choices aligned with their lifestyle needs.
Education should address specific concerns about oral absorption, emphasizing that fluoroquinolones, linezolid, and metronidazole achieve over 90% bioavailability. Patients benefit from learning that oral therapy reduces catheter-related bloodstream infection risks while allowing earlier hospital discharge and faster return to normal activities.
Healthcare providers should present outcome data showing a 2024 study found early switch to oral therapy for gram-negative bacteremia was associated with lower mortality (6.9% vs 14.3%) compared to prolonged IV treatment. This evidence-based approach to patient education supports shared decision-making and improves treatment adherence while challenging outdated assumptions about antibiotic administration routes.
How Can The Drip IV Infusion Help Guide Your Antibiotic Treatment Choice?
The Drip IV Infusion helps guide antibiotic treatment choices through evidence-based protocols that prioritize patient outcomes and safety. Modern antibiotic selection requires balancing efficacy, bioavailability, and individual patient factors. Healthcare providers at The Drip IV Infusion evaluate clinical stability, infection severity, and oral medication tolerance to determine optimal administration routes. The following personalized guidance and key takeaways inform treatment decisions in 2026.
Can The Drip IV Infusion Provide Personalized Guidance on IV vs Oral Antibiotics?
The Drip IV Infusion provides personalized guidance on IV versus oral antibiotics by utilizing AI-driven drug discovery systems that predict resistance patterns. These systems accelerate new antibiotic design while matching patients to optimal treatments based on pathogen susceptibility profiles. Advanced drug delivery systems using nanotechnology improve oral bioavailability of existing antibiotics, expanding oral therapy options for serious infections. Clinical pharmacists assess individual absorption capacity, drug interactions, and infection characteristics to recommend appropriate routes. Therapeutic drug monitoring ensures precise dosing adjustments for both IV and oral regimens. The Drip IV Infusion’s protocols incorporate the latest 2026 evidence showing oral antibiotics achieve equivalent outcomes for stable patients with high-bioavailability options.
What Are the Key Takeaways About Choosing IV vs Oral Antibiotics in 2026?
The key takeaways about choosing IV versus oral antibiotics in 2026 center on evidence supporting oral therapy for clinically stable patients. Studies from 2023-2026 demonstrate that transitioning from routine IV antibiotics to oral therapy reduces adverse events by 50% while maintaining treatment efficacy. Oral antibiotics with bioavailability exceeding 90%, such as linezolid, fluoroquinolones, and metronidazole, offer equivalent therapeutic outcomes for susceptible organisms. Cost analysis reveals oral therapy at $7 per day versus $65 for outpatient IV administration. Patient quality of life improves significantly with oral antibiotics through increased mobility and earlier hospital discharge. The paradigm shift toward oral antibiotics addresses antimicrobial resistance by reducing unnecessary IV exposure while optimizing clinical outcomes and healthcare resource utilization.