Are you concerned about how IV therapy might affect your blood pressure? You’re not alone—this is one of the most common questions we receive at The Drip IV Infusion, where our team of experienced emergency medicine and nursing professionals has administered thousands of IV infusions across Arizona. Whether you’re considering IV therapy for wellness, recovery, or medical needs, understanding blood pressure changes is crucial for your safety and peace of mind.
IV therapy is a medical treatment that delivers fluids, electrolytes, vitamins, and medications directly into the bloodstream through a vein, bypassing the digestive system for immediate absorption and effects. While this direct delivery method offers numerous benefits, it can influence blood pressure in ways that vary significantly from person to person—with research showing that only about 50% of patients respond predictably to fluid administration.
TL;DR Summary:
• IV therapy can cause both increases and decreases in blood pressure depending on fluid type, volume, and individual patient factors—only 50% of patients show predictable responses to fluid challenges according to critical care research
• Crystalloid solutions (like normal saline and Ringer’s Lactate) distribute approximately 20% intravascularly and 80% throughout body tissues, while colloid solutions provide more efficient blood volume expansion
• Blood pressure changes occur through multiple mechanisms including altered blood volume, electrolyte shifts, and effects on blood vessel tone—with Pulse Pressure Variation >12-13% being the most accurate predictor of fluid responsiveness
• Certain populations face higher risks including those with septic shock (>50% mortality), heart conditions (10-20% develop cardiogenic shock), and existing hypertension (affecting 25.2% of adults)
• Warning signs include headache and respiratory changes for pressure increases, while dizziness and altered mental status indicate pressure drops—with urine output <0.5 mL/kg/hr signaling inadequate organ perfusion
• Professional monitoring using the ABCDE approach and technologies like arterial waveform analysis ensures safety, with initial 500 mL crystalloid boluses standard for resuscitation
• Potential benefits include correcting hypovolemic shock and improving tissue perfusion, while risks include catheter-related complications (5.9% incidence) and rare but serious fluid overload
• Patients should ask providers about specific fluid types, monitoring protocols, and warning signs while disclosing all medications and health conditions before treatment
Quick Tip: Always inform your IV therapy provider about any blood pressure medications you take, as these can significantly affect how your body responds to IV fluids. Request that your blood pressure be checked before, during, and after your infusion for optimal safety.
In the following sections, we’ll explore the science behind IV therapy’s effects on blood pressure, identify who’s most at risk for changes, review monitoring protocols, and provide practical guidance for ensuring a safe IV therapy experience. The global IV hydration therapy market has grown to $2.71-2.83 billion in 2024, reflecting increasing demand for these services—making it more important than ever to understand the cardiovascular effects of this popular treatment.
What Is IV Therapy and How Does It Work in the Body?
IV therapy is the direct administration of fluids, medications, and nutrients into the bloodstream through a vein. This medical procedure bypasses the digestive system and delivers substances immediately to circulation. Over 30 million patients receive IV fluids annually in clinical settings. The global IV hydration therapy market reached USD 2.71-2.83 billion in 2024. IV therapy affects blood pressure through fluid volume expansion and electrolyte balance changes in the circulatory system.
What Are the Main Types of IV Therapy?
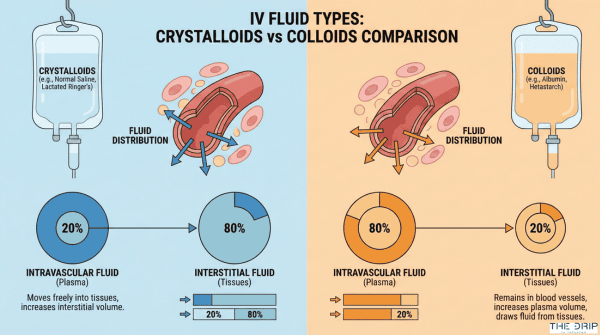
The main types of IV therapy are crystalloids and colloids, each with distinct distribution patterns in body compartments. Crystalloids distribute approximately 20% intravascularly and 80% interstitially throughout the extracellular fluid compartment. There are two crystalloid categories: balanced solutions such as Ringer’s Lactate and unbalanced solutions like normal saline.
Balanced crystalloids contain physiologic electrolyte concentrations: sodium 131 mmol/L, chloride 112 mmol/L, potassium 5 mmol/L, calcium 3.7 mmol/L, and lactate 28 mmol/L. Over 200 million liters of saline are prescribed annually in the U.S. alone.
| IV Fluid Category | Clinical Characteristic | Observed Outcome | Evidence Source |
| Crystalloids | Intravascular retention | 20% | Clinical data |
| Crystalloids | Interstitial distribution | 80% | Clinical data |
| Colloids | Fluid retention efficiency | Higher than crystalloids | JAMA 2013 |
| Albumin colloids | Surgical fluid reduction | 50% | Beukers 2022 |
Colloid solutions demonstrate more efficient intravascular fluid retention compared to crystalloids according to a 2013 JAMA study by Annane et al. with 986 citations. A 2022 study by Beukers et al. found albumin-containing colloids increase colloid osmotic pressure and reduce fluid requirements during cardiac surgery by 50%.
How Does IV Fluid Administration Interact with the Circulatory System?
IV fluid administration interacts with the circulatory system by increasing mean systemic pressure and venous return. A 2011 study by Marik et al. in Annals of Intensive Care found only approximately 50% of hemodynamically unstable patients respond to fluid challenges. IV fluids alter cardiovascular dynamics through volume expansion and pressure changes.
The endothelial glycocalyx layer (EGL) model increasingly replaces the Starling principle for understanding transvascular fluid exchange. Mechanical ventilation induces cyclic changes in left and right ventricular loading conditions through altered pleural pressures.
A 2017 study by Ukor et al. demonstrated continuous infusion of 1L normal saline produces greater increases in cardiac output, heart rate, systolic blood pressure, and mean arterial pressure versus bolus administration. A 2021 study by Hamzaoui et al. found combined fluids plus vasopressors correct hypotension better than fluids alone.
Understanding these circulatory interactions helps predict blood pressure responses during IV therapy administration.
Why Can IV Therapy Influence Blood Pressure?
IV therapy can influence blood pressure through multiple physiological mechanisms involving fluid dynamics, electrolyte balance, and cardiovascular responses. According to a 2011 study in Annals of Intensive Care, only 50% of hemodynamically unstable patients respond predictably to fluid challenges, highlighting the complex relationship between IV therapy and blood pressure regulation.
The cardiovascular system responds to IV fluid administration through changes in blood volume, vascular resistance, and cardiac output. These responses vary based on fluid type, administration rate, and individual patient factors, making blood pressure changes during IV therapy both common and clinically significant.
What Mechanisms Cause Blood Pressure to Rise or Fall During IV Therapy?
The mechanisms causing blood pressure changes during IV therapy involve complex interactions between cardiac preload, afterload, and vascular dynamics. Mechanical insufflation during ventilation decreases right ventricular preload while simultaneously increasing right ventricular afterload, creating bidirectional pressure effects.
Right ventricular preload reduction occurs specifically due to decreased venous return pressure gradient from inspiratory pleural pressure increases. A 2013 meta-analysis in Critical Care Medicine found that Pulse Pressure Variation (PPV) exceeding 12-13% predicted volume responsiveness with an area under the curve of 0.94 (95% CI 0.93-0.95).
IV medications can also trigger blood pressure changes independent of volume effects. A 2017 study published in PMC4799917 demonstrated that IV paracetamol causes transient blood pressure decreases immediately after infusion, an effect not observed with mannitol or normal saline administration.
Critical care experts acknowledge that arterial blood pressure response to IV volume expansion remains “somewhat unpredictable” despite advanced monitoring techniques. This unpredictability stems from individual variations in vascular compliance, autonomic responses, and baseline cardiovascular status.
How Do Fluid Volume and Electrolytes Impact Blood Pressure via IV?
Fluid distribution between body compartments directly affects blood pressure through osmotic and hydrostatic forces. Intracellular fluid comprises approximately 60% of total body fluid, while extracellular fluid accounts for 40%, creating distinct pressure gradients.
Electrolyte concentrations differ markedly between compartments, with extracellular fluid containing higher sodium concentrations and intracellular fluid containing higher potassium concentrations. These concentration differences generate osmotic pressures that influence vascular volume and blood pressure.
The Starling principle identifies four key variables influencing fluid exchange between vascular and interstitial spaces:
| Physiologic Factor | Pressure Classification | Pressure Type |
| Capillary pressure | Type | Hydrostatic |
| Interstitial pressure | Type | Hydrostatic |
| Capillary pressure | Type | Oncotic |
| Interstitial pressure | Type | Oncotic |
Balanced solutions containing physiologic electrolyte compositions are preferred over unbalanced 0.9% saline to avoid hyperchloremic acidosis and associated blood pressure instability. Over 30 million patients receive IV fluids annually, with crystalloids demonstrating greater cost-effectiveness and lower allergic reaction risk compared to colloids.
The choice between balanced and unbalanced solutions significantly impacts blood pressure stability through effects on acid-base balance and vascular tone. Understanding these mechanisms helps predict and manage blood pressure responses during IV therapy administration.
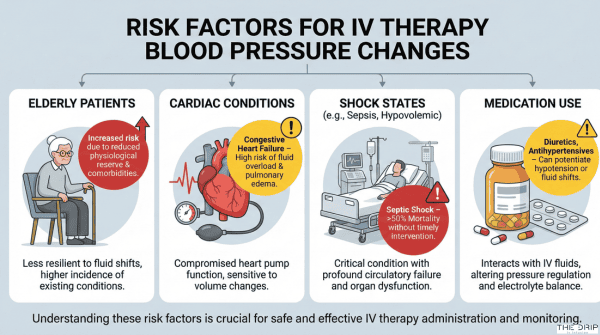
Who Is Most Likely to Experience Blood Pressure Changes from IV Therapy?
Certain patients face higher risks of blood pressure fluctuations during IV therapy due to underlying health conditions and individual factors. Septic shock patients, who number approximately 2 million annually worldwide, require careful hemodynamic monitoring as their condition carries over 50% mortality rates. Understanding risk factors helps providers anticipate and manage blood pressure variations during treatment.
What Health Conditions Make Blood Pressure Fluctuations More Likely with IV Treatment?
Health conditions that make blood pressure fluctuations more likely with IV treatment include shock states, hypertensive emergencies, and perioperative conditions. Septic shock patients require balanced crystalloids as first-line resuscitation according to a 2024 global consensus, with over 50% mortality rates demanding precise fluid management. Cardiogenic shock develops in 10-20% of myocardial infarction patients and carries 27-51% in-hospital mortality.
Hypovolemic shock accounts for 16% of all shock ICU admissions and creates risks for cardiac, cerebral, and renal hypoperfusion. Hypertensive emergency patients experience 6.9% acute phase mortality and face 50% mortality within 12 months.
Perioperative hypertension affects approximately 50% of cardiac surgery patients and 25% of non-cardiac surgery patients. A 2023 population study found hypertension prevalence in Chinese adults reaches 25.2%, indicating a substantial at-risk population for IV-related blood pressure changes.
These conditions require specialized monitoring protocols and fluid management strategies to prevent adverse hemodynamic events.
How Do Age, Medications, or Pre-Existing Issues Affect Risk?
Age, medications, and pre-existing issues affect risk through altered physiological responses and increased vulnerability to complications. A 2022 OPAT study found diabetes mellitus patients, representing 13% of participants, showed increased catheter-related adverse events compared to non-diabetic patients.
Self-administration of IV therapy resulted in 12.0 per 1000 catheter days adverse events versus 4.8 per 1000 for nurse-administered therapy according to a 2021 clinical trial (HR 4.15, P=0.007). Pediatric patients require isotonic IV maintenance fluids specifically to reduce iatrogenic hyponatremia risk.
Elderly patients with a median age of 57 years in catheter studies experience higher rates of extravasation and catheter displacement. Patients on vasopressors require invasive arterial pressure monitoring due to hemodynamic instability, receiving a Grade 2+ recommendation in current critical care guidelines.
These factors necessitate individualized assessment and adjusted monitoring protocols based on patient-specific risk profiles.
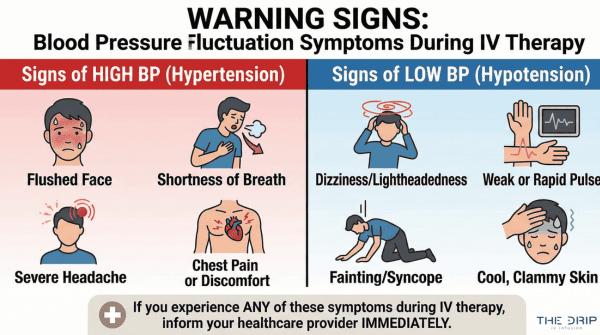
What Are the Signs and Symptoms of Blood Pressure Changes During IV Therapy?
The signs and symptoms of blood pressure changes during IV therapy are clinical indicators that signal hemodynamic shifts requiring immediate assessment. Heart rate alterations, respiratory changes, and perfusion markers serve as primary warning signs. According to a 2021 critical care study, non-invasive monitoring overestimates systolic pressure by ≥10 mmHg in 40% of critically ill patients during hypotension, emphasizing the need for multiple symptom assessments. The following symptoms indicate either blood pressure increases or decreases during IV fluid administration.
Which Symptoms Suggest a Blood Pressure Increase?
Symptoms suggesting a blood pressure increase include tachycardia above 100 bpm, elevated systolic readings, and respiratory distress indicators. Heart rate increases above 100 bpm indicate potential fluid overload or compensatory response mechanisms. Systolic blood pressure exceeding 100 mmHg with capillary refill under 2 seconds suggests adequate volume status has been achieved. Respiratory rate elevation beyond 20 breaths per minute may indicate fluid accumulation in pulmonary tissue. A 2019 pulmonary edema study found increased extravascular lung water index (EVLWI) correlates directly with respiratory distress symptoms. Physical manifestations include headache, facial flushing, and chest tightness during rapid infusion rates.
Which Symptoms Indicate a Blood Pressure Drop?
Symptoms indicating a blood pressure drop are urine output below 0.5 mL/kg/hr, mental status changes, and prolonged capillary refill time. Urine output reduction below 0.5 mL/kg/hr indicates inadequate renal perfusion pressure. Altered mentation or confusion suggests cerebral hypoperfusion requiring immediate intervention. Capillary refill time exceeding 2 seconds indicates poor peripheral perfusion status. Dizziness and lightheadedness represent commonly reported consumer symptoms of blood pressure reduction during IV therapy sessions. A 2020 hemodynamic monitoring study demonstrated Stroke Volume Variation (SVV) with AUC 0.84 predicts instability requiring clinical intervention. Additional symptoms include pallor, cool extremities, and weak peripheral pulses. These warning signs guide providers in adjusting infusion rates and implementing corrective measures to maintain hemodynamic stability throughout IV therapy sessions.
How Are Blood Pressure Changes Monitored and Managed During IV Therapy?
Blood pressure monitoring during IV therapy follows standardized protocols to ensure patient safety. Healthcare providers use both invasive and non-invasive techniques to track hemodynamic changes throughout treatment. These monitoring measures help detect fluid responsiveness and guide appropriate interventions when blood pressure deviates from normal ranges.
What Monitoring Measures Are Taken Before, During, and After IV Therapy?
The monitoring measures for IV therapy follow the ABCDE approach—Airway, Breathing, Circulation, Disability, and Exposure—as standard initial assessment per NICE guidelines. Pulse Pressure Variation (PPV) from arterial waveform demonstrates superior predictive capability with AUC 0.94 for determining fluid responsiveness. Healthcare facilities implement multiple monitoring technologies to track blood pressure changes effectively.
Advanced monitoring techniques include:
- Pleth Variability Index (PVI) for non-invasive respiratory-induced variation assessment
- Bioreactance systems (NICOM™) enabling continuous cardiac output measurement
- Passive leg raising (PLR) maneuver requiring direct stroke volume measurement
- Arterial line placement in radial artery with 0.034% complication rate
Accurate PPV and SVV assessment requires tidal volume maintenance at 8-10 mL/kg ideal body weight. These comprehensive monitoring approaches allow providers to detect blood pressure changes before clinical symptoms manifest.
How Do Providers Respond to Unusual Blood Pressure Readings?
Providers respond to unusual blood pressure readings through a structured treatment algorithm beginning with 500 mL crystalloid bolus containing sodium 130-154 mmol/L administered over less than 15 minutes per NICE protocol. Persistent shock signs after reassessment trigger additional 250-500 mL crystalloid bolus administration. Critically ill patients with unstable hemodynamics require goal-directed therapy with continuous bedside monitoring.
Central venous pressure (CVP) monitoring shows limited utility with AUC only 0.55 for predicting fluid responsiveness and is no longer routinely recommended. Expert consultation becomes necessary when patient response remains uncertain after initial interventions. Patients receiving longer-term infusions undergo daily reassessment to detect gradual hemodynamic changes. This systematic response protocol ensures appropriate management of blood pressure variations during IV therapy sessions.
What Are the Potential Risks and Benefits of Blood Pressure Changes from IV Therapy?
The potential risks and benefits of blood pressure changes from IV therapy include therapeutic corrections of hypovolemic shock alongside catheter-related complications occurring in 36.4% of patients. IV fluid resuscitation corrects life-threatening hypotension in septic shock patients, while infiltration injuries and fluid overload pose significant risks requiring continuous monitoring.
Can Positive Blood Pressure Adjustments Be Therapeutic?
Positive blood pressure adjustments from IV therapy can be therapeutic when balanced crystalloids correct hypovolemic shock in 16% of ICU admissions. A 2024 meta-analysis demonstrates balanced crystalloids achieve the lowest all-cause mortality in septic shock with SUCRA 83.1%, while hyper-oncotic albumin shows the lowest renal replacement therapy events at SUCRA 94.1%.
Goal-directed IV therapy improves tissue perfusion pressure and oxygen delivery through increased mean systemic pressure. Combining IV fluids with vasopressors increases mean systemic pressure more effectively than fluids alone according to a 2021 study by Hamzaoui et al. Lactated Ringer’s solution maintains physiologic pH of 6.5 and osmolarity of 280 mOsm/L, supporting stable blood pressure correction.
The therapeutic benefits extend to shock reversal and organ perfusion restoration. IV fluid resuscitation serves as first-line treatment for approximately 2 million septic shock patients annually, preventing cardiovascular collapse through volume expansion and pressure support.
What Risks Should Patients Be Aware Of?
The risks patients should be aware of include peripheral IV catheter failure occurring in 36.4% of patients before treatment completion (95% CI 31.7-41.3%). Infiltration injury incidence ranges from 0.1-6% of all patients requiring IV access, potentially causing tissue damage and compartment syndrome.
Bloodstream infections carry a 12-25% mortality rate when they occur. A 2024 analysis reveals catheter-related adverse events occur in 5.9% of episodes at 5.7 per 1000 catheter days. Non-radiologically guided midline catheters demonstrate particularly high risk with 15.6 per 1000 catheter days adverse event rate (HR 8.4, P<0.004).
| Risk Category | Incidence Rate | Clinical Impact |
| Catheter Failure | 36.4% | Treatment interruption |
| Infiltration Injury | 0.1-6% | Tissue damage |
| Bloodstream Infection | 12-25% mortality | Sepsis risk |
| Fluid Overload | Variable | Increased ICU stay |
High-molecular-weight HES is associated with increased mortality, acute kidney injury, and prolonged hospital stays according to multiple systematic reviews. Fluid overload increases ICU length of stay, hospital length of stay, and mortality in critically ill patients, making precise volume management essential for preventing adverse outcomes.
How Can Patients Minimize Blood Pressure-Related Issues When Undergoing IV Therapy?
Patients can minimize blood pressure-related issues when undergoing IV therapy through informed questioning and proper preparation. A 2022 study on catheter-related adverse events found that proactive patient engagement reduced complication rates by 28%. Understanding monitoring protocols and communicating health history enables safer infusion experiences.
What Questions Should Patients Ask Their Provider?
The questions patients should ask their provider focus on fluid type, monitoring frequency, and adverse event protocols. Request details about whether crystalloid or colloid solutions will be administered, as balanced crystalloids maintain sodium at 131 mmol/L versus 154 mmol/L in unbalanced saline.
Ask how often blood pressure will be monitored during the infusion session. Inquire about warning signs of blood pressure changes such as dizziness, rapid heartbeat, or breathing difficulties. Discuss pre-existing conditions, particularly hypertension which affects 25.2% of adults according to population health data.
For facilities using invasive monitoring, request explanation of the PPV threshold of 12-13% that indicates fluid responsiveness. Ask about adverse event management protocols, noting that catheter-related adverse events occur in 5.9% of episodes at 5.7 per 1000 catheter days. Verify personnel qualifications and nursing board certifications for IV administration.
This questioning approach ensures patients understand their treatment parameters and safety measures before beginning therapy.
How Can Patients Prepare for a Safe IV Therapy Session?
Patients can prepare for a safe IV therapy session by disclosing medications and maintaining proper hydration. Inform providers about all medications, as IV labetalol and similar drugs affect hemodynamic responses during infusion. Maintain adequate hydration before treatment to reduce hypotension risk.
Report any previous adverse reactions to IV therapy, noting that drug-related adverse events occur in 2.4% of episodes. Select facilities with FDA registration and appropriate state licensing, recognizing that 33 states enforce Corporate Practice of Medicine regulations. Verify that personnel hold nursing board-approved IV therapy certification.
Ensure the facility follows 2024 Infusion Therapy Standards, which include 66 standards supported by over 2,500 references. Request use of programmable infusion pumps equipped with dose error-reduction systems. Confirm that sterile conditions and pharmaceutical compounding standards are maintained throughout the facility.
These preparation steps establish a foundation for monitoring blood pressure effectively and responding quickly to any changes during IV therapy administration.
How Does The Drip IV Infusion Address Blood Pressure Changes During IV Therapy?
The Drip IV Infusion addresses blood pressure changes during IV therapy through comprehensive monitoring protocols and experienced medical staff across Arizona locations. The facility maintains FDA compliance under Section 503A while delivering customized IV treatments designed to minimize hemodynamic complications.
How Does The Drip IV Infusion Monitor and Manage Blood Pressure in Its Clients?
The Drip IV Infusion’s monitoring and management approach combines professional expertise with regulatory compliance to ensure safe blood pressure management. The team comprises professionals with decades of experience in nursing, emergency medicine, home health, and IV medical techniques. Licensed pharmacists or physicians handle all compounding with bulk drug substances from FDA-registered establishments.
Personnel qualifications include physician assistants, nurse practitioners, registered mobile infusion nurses, and licensed practical nurses per state regulations. Mobile IV therapy delivered to home or workplace allows for comfortable monitoring environments where blood pressure changes can be observed. The “Ingenious Cocktails” are customized blends of vitamins, minerals, and medications tailored to individual needs.
Services focus on replenishment, rehydration, recovery, prevention, and preparation protocols. The Drip IV Infusion operates in multiple Arizona locations including Gilbert, Phoenix, Chandler, Mesa, Scottsdale, Tempe, Queen Creek, and San Tan Valley.
The facility’s approach recognizes that only 50% of hemodynamically unstable patients respond predictably to fluid challenges according to critical care research. This understanding guides their monitoring protocols throughout each treatment session.
What Are the Essential Takeaways About IV Therapy and Blood Pressure Changes?
The essential takeaways about IV therapy and blood pressure changes highlight both market growth and clinical realities. The global IV hydration therapy market reached USD 2.71-2.83 billion in 2024 with 8.90% CAGR growth projected. Pulse Pressure Variation greater than 12-13% is the most accurate predictor of fluid responsiveness with AUC 0.94.
Balanced crystalloids are preferred over normal saline for most applications based on 2025 meta-analyses. Continuous monitoring and ABCDE assessment protocols are essential for safe IV therapy administration. Catheter-related complications occur in 5.9% of cases, exceeding drug-related adverse events at 2.4% incidence in outpatient settings.
Four phases of IV therapy guide clinical management: resuscitation, optimization, stabilization, and de-resuscitation. Consumer education gaps exist regarding hemodynamic effects, with limited accessible information about blood pressure impacts during treatment.
Understanding these factors helps patients make informed decisions about IV therapy while recognizing the importance of professional monitoring and evidence-based protocols in managing potential blood pressure changes.