Inflammation is a common process in human bodies. It is a natural immune system response that defends the body from harmful agents or foreign objects. There are many potential treatments, one of the most popular being IV therapy. With so many options available, you should know how to choose the best IV therapy for inflammation.
Finding the right solution for your medical issue involves understanding your symptoms and matching them with IV ingredients that may reduce inflammation. Let’s find out about the science behind using IV therapy for inflammation and discover the most effective supplement for inflammation!
Intravenous therapy infuses fluids such as vitamins, minerals and other nutrients directly into the bloodstream. IV therapy providers offer different cocktails, each with unique ingredients. Different IV therapy solutions are recommended for treating different conditions.
So, what IV therapy is good for inflammation? If you feel some symptoms of inflammation, there are several IV therapy options available that might reduce them. The best IV therapy for inflammation can be vitamin C therapy, glutathione therapy, magnesium therapy, or a Myers cocktail.
Vitamin C IV therapy
Vitamin C is an essential vitamin for normal body function. It has a multifold role in the system as it is involved in many processes, the most important being body tissue growth, development, and repair. It is also crucial for a strong and healthy immune system.
Considering that inflammation possibly damages healthy cells, vitamin C can protect immune cells during an inflammatory response. It may prevent intracellular ROS production and maintain tissue integrity.
Glutathione IV therapy can provide several health benefits, such as maintaining optimal health and protecting the body from toxins. Glutathione is a substance that may fight inflammation, because it potentially reduces oxidative stress.
Inflammation not only induces oxidative stress but also reduces the antioxidant capacity of the cells. Moreover, glutathione IV infusion can protect cells from inflammation and free radicals.
Magnesium IV therapy
If you are still unsure what IV drip is the right choice for inflammation, magnesium therapy may be an option. Magnesium is a beneficial mineral that can reduce inflammatory markers such as C-reactive protein and nitric oxide.
The Myers cocktail may boost your immune system, hydrate your body, and improve your energy level. Besides the well-known benefits, the Myers cocktail can be one of the best IV therapies for inflammation.
The exact nutrients contained within can vary slightly, depending on the provider. But generally, it should have the following:
Vitamin C
Vitamin B-12
B-complex
Zinc
Glutathione
Magnesium
The Myers IV therapy contains a unique mixture of anti-inflammatory agents, potentially offering a multifaceted approach to reducing inflammation throughout the body.
Are you wondering how effective is IV therapy for inflammation? The answer will depend on a number of factors, such as your overall health, age, and lifestyle. IV therapy, combined with exercise and a proper diet, may enhance your overall health and speed up recovery.
The latest recommendations for reducing inflammation are adequate levels of exercise and physical activity. Exercise can boost the immune system and allow for a proper bodily response to reduce inflammation. Activities as simple as aerobic exercise and walking can help you fight inflammation.
Other healthy habits that may increase the effectiveness of IV therapy for inflammation include:
Eating fatty foods
Getting enough sleep
Increasing food intake that is rich in antioxidants
Quitting smoking and alcohol
Reducing stress
Limiting sugar intake
Also, you may successfully fight inflammation by combining IV therapy with medication and supplements. If you are looking for the most effective supplement for inflammation, you might find it in some home remedies, such as:
Curcumin
Fish oil
Ginger
Resveratrol
Spirulina
Green tea extract
Bromelain
Garlic
Conclusion
What will be the best IV therapy for inflammation depends on your individual body’s needs. When browsing through the different IV therapy options, it is crucial to consider the type of inflammation you have.
So, targeted nutrient delivery, through intravenous therapy, and the integration of physical therapy and dietary adjustments may effectively manage and reduce inflammation. Take care!
Dehydration usually occurs when the body loses more fluids than it takes in, which may result in impaired metabolic processes. If this condition is severe, oral medications cannot help enough, so IV therapy is recommended for many patients. But why is IV therapy needed, and what is in an IV bag for dehydration?
Read on as this article will explore the composition of IV dehydration bags, the various components used and their application in medical practice.
The IV bag for dehydration combines water, glucose, electrolytes, and sometimes additional additives. The composition of the IV bag may vary depending on the patient’s health conditions and specific needs.
So, what does IV hydration consist of in particular? In the following content, you will find out the IV composition and the main characteristics of its components.
Water
Water is a major component of IV fluids. Its main role is to dissolve the remaining ingredients in the IV bag and deliver them into the bloodstream. Water may also play a key role in regulating body temperature, maintaining cellular functions, and optimizing metabolic processes.
Electrolytes
Are electrolytes included in an IV bag for dehydration? Besides water as the main component, electrolytes are essential for IV hydration therapy. These minerals dissolve in water to form ions necessary for various physiological needs. Electrolytes such as sodium, potassium, chloride, and bicarbonate may often be found in the IV bag.
Sodium: May play an important role in maintaining muscle and nerve function and helping regulate blood pressure.
Potassium: An important electrolyte that may support heart function and maintain the normal balance of fluids in the cell.
Chloride: Works with sodium to maintain fluid balance and osmotic pressure. It may also play an important role in the body’s acid-base balance.
Bicarbonate: May act as a buffer important in maintaining the pH of the blood, preventing it from becoming too alkaline or too acidic.
Glucose
Glucose, an integral part of the IV bag, might be a quick source of energy and help absorb electrolytes. This component may be especially important for patients who have problems consuming food and drinks.
Other additives
Depending on the patient’s specific medical condition, additional ingredients in the IV bag may be included. These components can include vitamins, medicines, and supplements.
Vitamins: Although combining IV fluids with electrolytes may be an ideal choice to combat dehydration, adding vitamins may speed up the recovery process. Certain vitamins, such as B-complex and vitamin C, may provide nutritional support and help maintain the immune system.
Medications: If a specific medical condition is to be helped, medications are included as an integral part of the IV bag. Consultation with your IV nurse is important regarding the type of medication, amount, and frequency of administration.
What type of solution is typically in an IV bag for dehydration? IV fluids for dehydration can be classified according to their osmolality, that is, the concentration of dissolved substances in the solution and the osmolality of the blood. In this regard, such fluids are divided into hypertonic, isotonic, and hypotonic.
Isotonic solutions
The main characteristic of isotonic solutions is that they have the same osmotic pressure as blood plasma. This composition allows isotonic solutions to maintain a balanced osmotic pressure with equal amounts of fluids inside and outside the cell.
In addition, these solutions may increase the intravascular volume in several conditions, such as metabolic acidosis, vomiting, diarrhea, etc. In this group of solutions, the most commonly used in medical practice are:
Normal saline (0.9% NaCl)
You may also find the normal saline solution under 0.9NaCL, NS or 9% normal saline. Such a solution easily passes through cell membranes and is generally an isotonic solution.
Due to this feature, normal saline may be used in several conditions, such as vomiting, diarrhea, bleeding, and even shock conditions. In addition, normal saline might also be used when administering blood.
However, this solution may cause excess fluid retention due to its high sodium content. So, caution should be exercised in patients with kidney complications and those with heart disease.
Lactated Ringer’s solution
Lactated Ringer’s is another of the most commonly used isotonic solutions in addition to normal saline. Such a solution is most often found in emergency rooms, ambulances and where emergency cases are treated.
Furthermore, it may be used in patients with extensive blood loss, burns or severe injuries. In some cases, lactated Ringer’s may be used as an alternative to normal saline.
On the other hand, this solution is not advised for patients with kidney complications because it contains potassium. If this condition is not addressed, hyperkalemia may occur.
Hypotonic solutions
The main characteristic of hypotonic solutions is that they move from the bloodstream and pass into the cell through a semipermeable membrane or from the extracellular space to the intracellular space. This solution may help with cellular dehydration by returning the water in the cell to its normal limits.
Also, it may be used in several conditions, such as ketoacidosis. In general, the most commonly used isotonic solutions in medical practice can be:
0.225% NaCl
0.45% NaCl
0.33% NaCl
2.5% dextrose in water
Hypertonic solutions
Unlike hypotonic solutions, where fluids are transferred from extracellular to intracellular spaces, hypertonic solutions have the opposite situation. In such solutions, water is drawn from the cells, instead of being taken in. Because of this feature, hypertonic solutions may be used in patients with low sodium levels.
However, the patient’s health status should be considered before administering such a solution. Hypertonic solutions are not recommended for patients with heart or kidney problems. The most commonly used hypertonic solutions in patients are:
What is in an IV bag for dehydration? Knowing this is important in planning medical treatment and patient care. So, the IV bag may contain electrolytes, glucose, water, and occasionally other additives.
Moreover, isotonic solutions may be used for general rehydration, while hypertonic and hypotonic solutions may be used in patients with electrolyte imbalances and cellular dehydration problems. Yet, before administering any medication, the patient’s health status, age, metabolism and physical activity should be considered.
So, before undergoing IV treatment, it is recommended that you discuss the benefits and possible risks of IV therapy with your healthcare provider. Take care!
IV therapy is known as a minimally invasive method that delivers the necessary vitamins, minerals, and nutrients through the bloodstream. Many decide on IV therapy in case of an energy boost, when dealing with jetlag, or in most cases if they suffer from dehydration or vitamin deficiency. But, not everyone knows the process of how to prepare for an IV therapy and what measures to take for smooth administration.
In this article, we will point out several important factors and tips to help you prepare for your IV therapy session.
How to Prepare for an IV
If you are wondering how to prepare for an IV therapy, there are several factors to remember. First off, start by asking questions. Inform yourself about anything related to the administration of IV, from who will administer it and how it may make you feel to what type of medication or fluid will be administered in the IV bag.
Before IV therapy, you should share your medical history records with your healthcare provider to help them understand your medical condition and reduce the risk of misdiagnosis or adding liquids you may be allergic to.
But there’s more to the process of preparation for an IV besides getting informed and sharing your medical history records to help your IV infusion go as smoothly as possible. From setting up the environment and dressing into something comfortable to keep yourself hydrated, there’s plenty to do before getting the IV administered.
If you have decided to receive mobile IV treatment, take care of the environment. For this purpose, choosing a quiet place to sit or lie down comfortably is ideal. Also, keep in mind the lighting in the room. Ensure the room is sufficiently lit for the healthcare provider to perform the procedure successfully.
Hydration
Although it may seem counterintuitive to hydrate before a treatment intended to rehydrate you, it’s a good idea to drink plenty of water before the procedure. Ideally, we recommend you drink plenty of fluids 24 hours prior to the date of the appointment.
If your body is dehydrated there’s a high chance to better respond to IV therapy. If you are dehydrated, the veins contract, making it difficult for the healthcare provider to administer the IV therapy. On the other hand, if you are sufficiently hydrated, the veins become more dilated which makes the nurse’s task easier to find the vein on the first try.
A tip from our experienced team is to add salt to the water, as the water helps the body retain more moisture in your blood.
Source: shutterstock.com / Photo Contributor: New Africa
Eat before the treatment
You should avoid going for IV therapy on an empty stomach. It’s good to have a hot meal an hour or two before IV therapy. Eating a balanced meal before the therapy that contains plenty of water and proteins could help you prevent any side effects you may experience if you were to receive the IV therapy on an empty stomach.
Eating may help you avoid irritating symptoms during IV therapy, such as nausea, vomiting, and dizziness. If you have eaten before the procedure, your blood vessels will be more open, allowing the IV fluids to access the deepest tissues in the body.
Choose comfortable clothes that will not interfere during the administration. Wear clothing that will leave the internal veins open so that the health care provider can perform their task smoothly.
Source: shutterstock.com / Photo Contributor: Studio Romantic
Mental Preparation
If you feel afraid of the IV procedure, there are several techniques that you can use to overcome your fear. Take deep and slow breaths to help relax your body and mind, and engage in calming activities like meditation to help you relax before IV therapy. If you still feel uncomfortable once the IV therapy is administered, put on your headphones to get your mind somewhere else.
The duration of the IV procedure depends on the type of IV fluid being administered. This kind of therapy typically lasts an hour. In addition, there is a monitoring period when the healthcare provider checks that the IV therapy went well.
It is best to bring entertainment sources to help you pass the time more easily. For this purpose, you can read a book, listen to a podcast or music, or engage in game activities on your smartphone.
During the procedure, monitor the injection site and notify the medical team if you notice any changes or discomfort. Such changes may refer to swelling, pain, discoloration, or leaking.
After the procedure is over and the IV bag gets removed, you may experience minor pain at the injection site. You should report it to your healthcare provider if bruising occurs or persists for a long time.
Conclusion
Now that you know how to prepare for an IV, you will be able to reduce the fear and anxiety that can appear before and during IV therapy. In addition, be sure to communicate with your healthcare provider about the procedure and seek help immediately if you notice anything unusual related to IV therapy.
Intravenous therapy has advanced and become a popular choice among many target groups, including people doing sports recreationally or professionally. If you are one of them, you might be wondering does IV therapy help athletic performance.
Today there are available a variety of IV therapy cocktails containing different nutrients, allowing you to choose the best one for your needs. Some IV cocktails are advertised for boosting your energy, while others focus on speeding up your recovery. But do they actually influence the sports performance? Let’s find out.
Does IV Therapy Help Athletic Performance
In recent years, athletes have been leveraging the IV therapy benefits to rehydrate before exercising or during the recovery process. But does IV therapy help athletic performance?
Generally looking, high-quality and specially created IV therapy cocktails might improve your athletic performance. However, to feel the benefits you should research the IV solutions offered and find a reliable mobile IV for athletic performance provider.
To increase your chances of having the best outcome from mobile IV therapy, you should consult with the provider and explain what you expect from the treatment. With IV therapy, typically, you have two universal options:
Pre-workout IV therapy
Recovery IV therapy
In addition, with some IV therapy providers, you can customize the nutrients, vitamins, and fluids in your IV bag according to your needs and desired outcomes.
Source: shutterstock.com / Photo Contributor: muse studio
How Does IV Therapy Help Improve Athletic Performance
IV therapy might improve your athletic performance by providing your body with the needed vitamins, nutrients, and fluids for that activity. So, why is IV therapy good for athletes? Depending on the ingredients, IV therapies might help with:
Electrolyte replenishment and hydration
Nutrient infusion
Recovery and muscle repair
Electrolyte replenishment and hydration
When you exercise, your body produces sweat. In medical terms, sweat production means your body loses water and electrolytes.
As an athlete who is physically active, your body might need fluids and electrolytes in order to achieve your best athletic performance. Electrolyte replenishment through IV therapy provides you with salt and minerals. They contribute to the normal function of your body, prevent hypohydration, cardiovascular and thermal strain, and decrease aerobic performance.
In the group of minerals, athletes need potassium, magnesium, calcium, and phosphate. Aligning with the needs of the athletes and their increased physical activity, there are IV therapy solutions that contain saline and minerals for hydration and replenishment.
Nutrient infusions
The nutrition needs of an athlete are not the same as those of a person with normal physical activity. According to the Academy of Nutrition and Dietetics, athletes need vitamins and minerals to have enough energy, enhance their performance, and have good bone health.
Energy production
While a healthy diet is the best way to get all the nutrients your body needs, you might also benefit from IV therapy. To assist in your energy production, IV therapies typically contain different types of vitamin B. Vitamin B1, B2, B3 (niacin), B5 (pantothenic acid), B6 (pyridoxine), B7 (biotin), and vitamin B12 are crucial in the process of energy production.
In addition, other nutrients that are essential ingredients in IV therapy that might improve your energy levels are:
Vitamin C
Iron
Magnesium
Athletic performance
Still contemplating how does IV therapy benefit athletic performance? When athletes want to enhance their performance, they are advised to take nutrients such as vitamin B12, iron, and vitamin A.
Intravenous therapy is one of the quickest ways your body can get the nutrients it needs. The administering of nutrients is also a popular choice because it has high absorption rates, which may maximize the effects of the treatment.
To enhance the results from the administration of vitamins and minerals, athletes may improve their performance by consuming enough proteins, carbohydrates, calories, and fluids. The recommended amount generally depends on the type of sport and the frequency and the duration of your training.
There is no doubt that as athletes exercise, they are contributing to better bone health. However, athletes still might have lower bone mineral density, making them a high-risk group for bone stress injuries.
Vitamin D and calcium play a crucial role in athletes’ bone health. Other nutrients that are good for the skeletal system are potassium, magnesium, vitamins K, vitamin C, folic acid, and sodium. An athletic IV therapy with the right ingredients might also improve your bone health.
Recovery and muscle repair
The recovery period is extremely important because it prepares you for your next endeavor. Your body needs time and nutrients to recover and heal properly after an extensive workout or a competition.
During the recovery period, the focus is on your muscles. More specifically, your muscle system needs rest and nutrients to reduce the inflammation and restore its strength and function.
IV therapy in athletes is also used because it may promote faster recovery and muscle repair during the post-exercise process. IV therapies have carefully picked ingredients that might speed up the process, such as:
Vitamin C
Vitamin B12
Zinc
Taurine
NAC
Pyridoxine
Source: shutterstock.com / Photo Contributor: ra2 studio
The Do’s and Don’ts of IV Therapy for Athletic Performance
Now that you know whether does IV therapy help athletic performance, you might have other questions in mind, such as do pro athletes get IVs, or can I workout after IV therapy. Before you start looking for an athletic IV therapy provider, you should get familiar with the do’s and dont’s of the treatment.
Firstly, you should be aware that the World Anti-Doping Agency doesn’t allow athletes to get intravenous therapy higher than 100 milliliters in a 12-hour period. Whether you will be obligated to apply for TUE approval depends on the substances the IV therapy contains.
All in all, WADA only regulates the substances that athletes are allowed to get through intravenous administration and the amount they can get in a certain period of time. That doesn’t mean they are forbidden entirely. Consequently, there is a high percentage of both professional and amateur athletes that leverage the benefits of IV therapy.
And lastly, to answer one of the most common dilemmas, working out after IV therapy is generally allowed and safe. After all, there are special IV bags that are designed for administering before working out, as they might help with your athletic performance. On this topic, the medical professional administering the IV therapy can give you the most precise answer because they will monitor your well-being during the treatment.
Conclusion
IV therapy may be beneficial in many cases since it directly provides the body with the nutrients it requires. One of the most popular IV solutions is created for athletes. But does IV therapy help athletic performance? We hope that this scientific approach has solved this dilemma and you can now decide whether IV therapy will help you achieve your personal goals.
IV treatment may be one of the effective ways to deliver the necessary vitamins, minerals and nutrients directly into the bloodstream. There are several types of IV therapy that may be confusing for people, such as IV push and bolus. So, what are the key differences between IV push vs bolus?
Although both IV treatments might have the role of fast and efficient delivery of the necessary nutrients, several factors still differentiate them. So, read on as we break down the similarities and differences between these two popular types of IV therapy.
IV Push vs Bolus
IV push involves administering a concentrated dose of liquid or medication directly into the bloodstream for a few seconds to a minute. To perform this method, a medical nurse uses a syringe.
Unlike an IV push, an IV bolus is a rapid administration of a larger amount of fluid or medicine into a vein over a longer period. Typically, administration with this IV therapy might take up to five minutes, depending on the patient’s health condition.
Generally speaking, both types of therapy fall under the category of intravenous treatment, which means that the IV fluid is administered directly into the bloodstream while bypassing the digestive tract. Although such treatments are usually prescribed in hospital conditions, today, healthcare facilities offer mobile infusion services.
Source: shutterstock.com / Photo Contributor: Rob Byron
IV push administration
Appropriate equipment is required to perform this procedure. There is a syringe pre-filled with IV fluid, an IV access point such as a plug or IV catheter, syringes for flushing with saline, and antiseptic pads for sterilization.
An IV push is a procedure performed by a certified nurse who carefully pushes the contents of a syringe into a vein. During the entire administration, your health condition should be monitored.
This type of IV therapy is usually given to patients who need immediate attention or are in a life-threatening condition. So, heart medications, antibiotics, pain or anti-nausea medications may be administered with an IV push.
Usually, this type of IV therapy may be used in several cases. They are heart attack, anaphylactic shock, allergic reactions or other life-threatening conditions.
Bolus administration
IV bolus is a type of IV treatment where a large amount of fluid or medication is administered over a short period of time. This type of treatment uses an open fluid line. With an IV bolus, the contents of the IV bag may enter the body much faster.
Furthermore, certain equipment is required to perform this therapy, such as a bag with IV fluid and a tube connected to a syringe through which the fluid is administered. The entire procedure, on average, lasts from 15-20 minutes and depends on the amount of IV fluid administered. Also, constant flow rate monitoring is required to prevent possible IV fluid overload during the procedure.
IV bolus, as opposed to IV push, is usually recommended unless the patient is in a life-threatening condition. The most common example where this type of IV therapy is used is in patients with type 1 diabetes. In such patients, insulin is administered, an important factor in the fight against high blood sugar levels.
Key Differences Between IV Push and Bolus
While we have already discussed some of the fundamental distinctions between IV push and IV bolus, we will go into more detail about these two IV therapies in the following sections. Namely, IV push and IV bolus might differ by:
Delivery rate and volume
IV push involves administering a small amount of IV fluids over a rapid period of seconds to a minute. On the other hand, the IV bolus involves the administration of a larger volume of IV fluid that is administered for a longer time.
Patient safety
Carefully administering an IV push is essential for success since rushing the process might result in adverse consequences, including hypersensitivity or cardiovascular problems. The volume of IV fluid given should be carefully considered while administering IV bolus.
IV fluid excess might cause an electrolyte imbalance. This is especially important in individuals with heart disease and renal problems.
Nursing considerations and monitoring
An IV push should only be performed by nurses who have prepared the IV fluid to fit the IV line. In addition, constant monitoring is required during administration (heart rate and blood pressure monitoring).
Nurses should examine the administration volume while doing IV boluses to avoid excess IV fluid. During IV bolus administration, fluid and electrolyte status should be monitored to prevent IV fluid overload promptly.
There are a few things to remember, whether it’s an IV push or an IV bolus. We provided several important factors that you should know before undergoing IV therapy. Here are some of them:
Consultation with a doctor: A conversation with your doctor will help you familiarize yourself with the course of the procedure, the method of administration and possible risks.
Medical history: You should disclose all past and present medical conditions to your healthcare provider before IV therapy. That way, your healthcare professional will determine the appropriate IV treatment for you.
Allergic reactions: They are particularly important when dealing with IV push or IV bolus. So, emphasize all allergens to avoid possible risks and complications while administering the IV fluid.
Nutrition: You should also consider your food before the IV treatment. For this purpose, it is best to eat light foods that might not raise the blood sugar level.
Conclusion
Although there are differences between IV push vs bolus, they potentially represent one of the most efficient ways to administer IV fluids relatively quickly. To sum up, IV push distributes a concentrated dosage quickly via syringe, whereas IV bolus administers a greater quantity over a longer period, depending on the patient’s condition.
However, it is advisable to consider the aspects mentioned in the article before undergoing any of these IV treatments. Also, talking with your doctor is key to a successful procedure and maximizing the effects of IV therapy.
Regular intake of fluids and nutrients is important to maintain homeostasis in the body and establish balance. With the occurrence of injuries or diseases, this homeostasis can be disturbed, reducing the function of organs and metabolic processes. As a solution to this problem, many health professionals opt for crystalloids or colloids. So, what is the difference between crystalloid vs colloid?
In this article we will look at the main differences between these two solutions and their use for establishing normal bodily homeostasis.
Source: shutterstock.com / Photo Contributor: New Africa
Crystalloid vs Colloid
Fluids for infusion can be divided into two categories – colloids and crystalloids. Crystalloids are plasma volume expanders containing electrolytes such as potassium and sodium. Such crystals are able to dissolve in a solution and enable such a solution to move across membranes. Crystalloids are usually used to increase the intravascular volume when it is reduced.
Colloids, on the other hand, are gelatinous solutions that act as plasma volume expanders. Unlike crystalloids, the particles of colloids are too large to pass through semi-permeable membranes such as capillary membranes. Therefore, colloids remain in the intravascular space longer than crystalloids. An example of colloids are dextran, hydroxyethyl starch, albumin, and Haemaccel.
It’s worth noting that both solutions are administered in the IV hydration Arizona.
Crystalloid solutions
Medical professionals widely use crystalloids to maintain homeostasis and replace lost electrolytes. Such solutions are composed of water and electrolytes, which makes them suitable for improving the electrolyte and fluid imbalance in the body. The most common crystalloids used for IV hydration are:
Sodium chloride
Normal saline solution (0.9% sodium chloride), or physiological saline solution, is the most common crystalloid used in clinical practice. Due to its composition, it has a similar tonicity to the extracellular fluid.
Normal saline is commonly used for drug administration, fluid resuscitation, and intravascular volume expansion.
Ringer’s lactate solution
Ringer’s lactate (RL) solution is a mixture of sodium chloride, calcium chloride, potassium chloride, and sodium lactate in water. This mixture is usually administered in case of surgery, dehydration, or receiving medications through IV. In addition, this solution can be used in mild metabolic acidosis because it has the ability to metabolize lactate in the liver.
Hartmann’s solution
Hartmann’s solution (Compound Sodium Lactate) is similar to lactated Ringer’s solution except that it contains sodium bicarbonate in its composition. In addition, this solution is isotonic and provides electrolytes that have concentrations similar to the extracellular fluid.
When it comes to use, Hartmann’s solution is used for fluid resuscitation, especially in cases of hypovolemia and dehydration, as well as perioperative fluid management.
Hypertonic saline
Unlike normal saline, which may contain 3% or 5% sodium chloride, hypertonic solutions contain a higher concentration of sodium chloride. Regarding its use, such solutions have specific uses in cases such as hyponatremia, hypovolemic shock, and treating cerebral edema.
In addition, hypertonic solutions are characterized by an osmotic effect. With this property, these solutions draw water from the interstitial and intracellular compartments into the intravascular space, thus increasing the intravascular volume by improving perfusion.
Colloid solutions
Colloid solutions are used to replace lost fluids to increase intravascular volume by increasing oncotic pressure in the bloodstream.
Unlike crystalloids, colloids contain larger molecules suspended in a liquid base, allowing fluid to be retained in blood vessels. In the following, we will look at some of the colloidal solutions that are most often used in medical practice:
Albumin solutions
Albumin solutions are one of the most used colloidal solutions in clinical practice. Namely, albumin is a natural protein found in plasma that increases intravascular oncotic pressure.
Such solutions are usually available in various concentrations, such as 5% and 25%. They are used in patients with hypoalbuminemia, hypovolemia and in those conditions where expansion of the plasma volume is required.
Hydroxyethyl starch
Hydroxyethyl starch is a synthetic starch commonly used for fluid resuscitation to replace intravascular pressure. This colloidal solution has different molecular weights and concentrations, affecting pharmacodynamic and pharmacokinetic properties.
When it comes to its use, hydroxyethyl starch is most commonly used for hypovolemic shock and critically ill patients.
Gelatin solution
Gelatin-based colloidal solutions are composed of hydrolyzed gelatin derived from animal sources. Such solutions are used for volume replacement in those situations requiring rapid intravascular expansion, usually in surgery or trauma.
Although such solutions are well tolerated, caution should be exercised in their application in persons with a history of sensitivity to gelatin.
Differences Between Crystalloid and Colloid Solutions
When choosing a solution to replenish lost fluids, one should know what distinguishes crystalloids and colloids. So, what is the difference between a colloid and a crystalloid?
Molecular size and properties – Crystalloids comprise small molecules such as ions and small solutes, while colloids consist of larger molecules suspended in solution.
Volume expansion capabilities – Crystalloid solutions can effectively expand intravascular volume, and their effect is short-lived. On the other hand, colloids expand the volume by increasing the intravascular volume and have a longer effect.
Duration of intravascular retention – Crystalloids have a relatively short duration of intravascular retention in contrast to colloids, which in turn have prolonged retention due to the size of the molecules.
Hemodynamic effects – Crystalloids expand plasma volume by replenishing fluid deficits. On the other hand, colloids increase intravascular volume by increasing oncotic pressure.
Potential adverse effects and complications – When it comes to adverse effects, crystalloids are generally safe to use. But when crystalloids are administered in large volumes, it may lead to electrolyte imbalance, tissue edema or dilutional coagulopathy. On the other hand, the negative effects of colloid solutions may include allergic reactions, tissue edema, and coagulopathy.
Ready for Better Hydration with IV Therapy ?
Professional hydration therapy ensures that the right fluids are administered safely and effectively. For individuals seeking convenient, on-demand care, mobile IV therapy brings hydration and recovery directly to their location in Gilbert.
Can You Get Mobile IV Therapy in Gilbert for Hydration and Recovery?
Yes, you can get mobile IV therapy in Gilbert for hydration and recovery, making treatment convenient and personalized. Mobile IV therapy in Gilbert delivers fluids directly to your home, workplace, or event, helping restore balance with the right mix of crystalloid and colloid solutions when needed. Whether you need rapid hydration, recovery after illness, or support for conditions like dehydration and fatigue, our licensed professionals ensure safe and effective care. Learn more about [Mobile IV Therapy in Gilbert] to see how it can support your wellness and recovery.
Is Understanding Crystalloids vs Colloids Essential for IV Therapy?
Yes, understanding crystalloids vs colloids is essential for IV therapy because it helps patients and providers choose the most effective treatment. By knowing the differences in fluid retention, electrolyte balance, and plasma volume expansion, you can better appreciate how IV therapy supports hydration and recovery. When comparing these two solutions, remember there is no one-size-fits-all solution for all patients. Both solutions come with their advantages, and the choice depends on several factors, such as the patient’s health condition, clinical scenario, and available resources.
However, when administering such solutions, healthcare professionals should consider the patient’s individual needs as well as the potential risks that may arise during their administration.
IV vitamin C is a method of delivering ascorbic acid directly into the bloodstream through intravenous infusion, bypassing intestinal absorption limits entirely. Elevated plasma levels are temporary; the kidneys restore baseline concentrations within hours, with complete renal clearance occurring within 24 hours even at high doses.
This guide covers IV vitamin C pharmacokinetics and absorption, duration across different populations, factors that influence clearance speed, infusion frequency guidelines, and safety considerations.
IV vitamin C achieves plasma concentrations up to 70 times higher than oral supplementation allows, but renal excretion begins rapidly once levels exceed the body’s saturation threshold. The half-life of circulating ascorbic acid ranges from roughly 8 to 16 hours under normal conditions, with first-order pharmacokinetics governing elimination at doses up to 75 g.
How long vitamin C remains active varies significantly by population. Immunocompromised individuals, athletes, and older adults all deplete stores faster due to heightened oxidative stress, metabolic demand, or low baseline levels. Smokers carry serum concentrations one-third lower than nonsmokers, and surgical patients experience a 39% plasma depletion during the first postoperative week.
Dosage size, kidney function, hydration status, and metabolic rate each shape clearance speed differently. Well-hydrated individuals with healthy kidneys clear vitamin C faster, while illness and infection accelerate tissue consumption before renal excretion even becomes the primary factor.
Optimal infusion frequency depends on the goal: weekly sessions during acute recovery, biweekly for immune support, and monthly for general wellness. Pre-treatment screening for G6PD deficiency and kidney conditions remains essential for safe administration.
What Is IV Vitamin C and How Does It Work?
IV vitamin C is a method of delivering ascorbic acid directly into the bloodstream through intravenous infusion, bypassing the digestive system entirely. The sections below explain how this differs from oral supplementation and what happens once vitamin C enters your blood.
How Does Intravenous Vitamin C Differ From Oral Vitamin C?
Intravenous vitamin C differs from oral vitamin C primarily in absorption and achievable plasma concentration. Oral doses are subject to intestinal absorptive control; the body absorbs 100% of vitamin C at doses up to 200 mg, but efficiency drops progressively above 500 mg. Plasma levels from oral intake plateau between 60 and 80 micromoles per liter in healthy adults, with a hard ceiling below 300 μM.
Intravenous administration bypasses this intestinal regulation entirely. According to the National Cancer Institute, IV delivery can raise plasma vitamin C concentrations up to 20 mM, roughly 70 times higher than the oral maximum. Within hours, however, renal excretion begins restoring levels to baseline.
This pharmacokinetic gap matters most for individuals already depleted. Smokers carry serum concentrations one-third lower than nonsmokers, and surgical patients experience a 39% plasma depletion during the first postoperative week. For these populations, oral supplementation alone often cannot restore adequate levels fast enough.
What Happens to Vitamin C Once It Enters Your Bloodstream?
Vitamin C enters the bloodstream and immediately distributes to tissues with the highest metabolic demand, including the adrenal glands, brain, and immune cells. As an antioxidant, L-ascorbic acid neutralizes free radicals and supports collagen synthesis throughout the body.
The kidneys regulate circulating levels through the renal threshold. Once plasma concentration exceeds this threshold, excess vitamin C is filtered and excreted in urine. At doses up to 75 g, intravenous vitamin C follows first-order pharmacokinetics, meaning clearance rate increases proportionally with concentration. At 100 g doses, complete renal clearance occurs within 24 hours.
Because the body cannot store large reserves of this water-soluble nutrient, tissues absorb what they need quickly while the kidneys eliminate the surplus. Understanding this clearance timeline helps explain how long IV vitamin C remains active in your system.
How Long Does IV Vitamin C Stay in Your System?
IV vitamin C stays in your system for a limited window before the kidneys clear it. How long it lasts depends on your health status, age, and activity level. The following sections break down duration for healthy adults, immunocompromised individuals, athletes, and older adults.
How Long Does IV Vitamin C Last in Healthy Adults?
IV vitamin C lasts in healthy adults for several hours at elevated plasma levels before renal excretion returns concentrations to baseline. According to pharmacokinetic research published in PMC (Chen et al., 2022), intravenous vitamin C exhibited first-order pharmacokinetics at doses up to 75 g, with complete renal clearance demonstrated at 100 g within 24 hours.
In practical terms, this means the therapeutic window is relatively brief. The kidneys begin filtering excess ascorbic acid almost immediately once plasma saturation exceeds the renal threshold. For most healthy adults with normal kidney function and adequate hydration, peak plasma concentrations decline steadily within the first few hours post-infusion.
How Long Does IV Vitamin C Last in Immunocompromised Individuals?
IV vitamin C lasts in immunocompromised individuals for a shorter effective duration than in healthy adults. The body consumes ascorbic acid more rapidly when fighting infection or managing chronic inflammation. As reported in a review published in Nutrients (MDPI), infections significantly impact vitamin C levels due to enhanced inflammation and metabolic requirements, and treatment of established infections requires gram doses of the vitamin to compensate for increased metabolic demand.
Because oxidative stress depletes circulating vitamin C faster, immunocompromised individuals often reach baseline plasma concentrations sooner after infusion. This accelerated utilization is why higher or more frequent dosing is sometimes considered for this population under clinical guidance.
How Long Does IV Vitamin C Last in Athletes or Active People?
IV vitamin C lasts in athletes or active people for a potentially shorter duration compared to sedentary individuals. Intense physical activity generates oxidative stress through free radical production, which increases the body’s demand for antioxidant capacity. Vitamin C, as L-ascorbic acid, is consumed more quickly during and after strenuous exercise to neutralize these free radicals and support collagen synthesis for tissue repair.
Athletes with higher metabolic rates process nutrients faster overall, meaning plasma vitamin C concentrations may decline more rapidly after infusion. For active individuals seeking sustained benefits, timing infusions around training cycles can help maximize the therapeutic window.
How Long Does IV Vitamin C Last in Older Adults?
IV vitamin C lasts in older adults for a variable duration, often complicated by lower baseline stores and reduced physiological efficiency. According to research published in Nutrients (MDPI), lower mean vitamin C status has been observed in both free-living and institutionalized elderly people, and low vitamin C concentrations below 17 µmol/L in individuals aged 75 to 82 years are strongly predictive of all-cause mortality.
Because older adults frequently start from a depleted baseline, infused vitamin C may be utilized more quickly to replenish tissue stores rather than maintaining elevated plasma levels. Reduced kidney function, common in aging, can also alter clearance rates in either direction. This makes individualized assessment especially important for older populations considering IV vitamin C therapy.
Understanding how different populations metabolize IV vitamin C helps determine the right infusion frequency for lasting benefits.
What Is the Half-Life of Vitamin C in the Body?
The half-life of vitamin C in the body ranges from approximately 8 to 16 hours under normal physiological conditions, though this window shifts based on dose, health status, and route of administration. After intravenous delivery, plasma concentrations peak far higher than oral intake allows, but renal excretion works rapidly to restore baseline levels.
According to pharmacokinetic research published in PMC (Chen et al., 2022), intravenous vitamin C exhibited first-order pharmacokinetics at doses up to 75 g, with complete renal clearance occurring within 24 hours at 100 g doses. This means even large IV doses follow a predictable elimination curve where the kidneys filter excess ascorbic acid efficiently once plasma saturation exceeds the renal threshold.
Several factors compress or extend this half-life window:
Oxidative stress and infection accelerate vitamin C utilization, effectively shortening its functional half-life as tissues consume it faster than normal.
Kidney function directly governs clearance speed; impaired renal filtration slows excretion and extends circulation time.
Baseline plasma levels matter because individuals starting with depleted stores retain a higher percentage of the infused dose.
Metabolic rate influences how quickly tissues draw vitamin C from the bloodstream for collagen synthesis, antioxidant activity, and immune function.
For practical purposes, most of an IV vitamin C dose has either been utilized by tissues or excreted by the kidneys within 24 hours. The steepest decline in plasma concentration happens during the first few hours post-infusion as renal excretion restores vitamin C to baseline levels. This rapid clearance pattern is precisely why understanding infusion frequency matters for sustained benefits.
What Factors Affect How Long IV Vitamin C Remains Active?
Several factors affect how long IV vitamin C remains active, including dosage size, kidney function, hydration status, and metabolic rate. Each variable influences plasma clearance differently.
How Does Dosage Size Influence Duration in the Body?
Dosage size influences duration in the body by determining how long the kidneys take to restore plasma vitamin C to baseline levels. Larger infusions produce higher peak plasma concentrations, which means renal excretion must work longer to clear the surplus. According to a 2022 pharmacokinetic study published in PMC, intravenous vitamin C exhibited first-order pharmacokinetics at doses up to 75 g, while a 100 g dose demonstrated complete renal clearance within 24 hours. Smaller doses clear faster because the kidneys reach the renal threshold sooner. This relationship between dose and clearance time is why practitioners tailor infusion amounts to each client’s specific wellness goals.
How Does Kidney Function Affect Vitamin C Clearance?
Kidney function affects vitamin C clearance because the kidneys serve as the primary elimination pathway for circulating ascorbic acid. Healthy kidneys filter excess vitamin C efficiently, restoring plasma levels to baseline within hours after an infusion. When renal function is impaired, this filtration slows, allowing vitamin C to remain in circulation longer but also increasing the risk of complications. Individuals with kidney disease or a history of kidney stones require careful medical evaluation before receiving high-dose IV vitamin C. Compromised renal clearance can lead to oxalate accumulation, making pre-infusion kidney assessment an essential safety step.
How Does Hydration Status Change Vitamin C Retention?
Hydration status changes vitamin C retention by directly influencing blood volume and renal filtration rate. Well-hydrated individuals maintain higher glomerular filtration rates, which accelerates the clearance of water-soluble nutrients like ascorbic acid from plasma. Dehydration reduces kidney filtration efficiency, potentially slowing vitamin C excretion and extending its presence in the bloodstream. However, this slower clearance does not necessarily mean greater cellular benefit, since tissues still absorb vitamin C at their own saturation-dependent rate. Proper hydration before and after an IV infusion supports predictable pharmacokinetics and helps the body process vitamin C at a steady, efficient pace.
How Do Metabolic Rate and Activity Level Impact Duration?
Metabolic rate and activity level impact duration by increasing the body’s consumption of vitamin C during periods of heightened physiological demand. Higher metabolic rates, whether from exercise, fever, or physical labor, accelerate ascorbic acid utilization for tissue repair and antioxidant defense. According to a review published in Nutrients (MDPI), infections significantly impact vitamin C levels due to enhanced inflammation and metabolic requirements, and treatment of established infections requires gram doses to compensate for the increased metabolic demand. Athletes and highly active individuals tend to deplete circulating vitamin C faster than sedentary individuals. For those with elevated metabolic needs, more frequent infusions may help maintain optimal plasma levels over time.
How Quickly Does Your Body Use Up IV Vitamin C?
Your body uses up IV vitamin C at different rates depending on physiological demand. Illness, oxidative stress, and normal metabolic function each consume ascorbic acid at distinct speeds.
How Fast Is Vitamin C Used During Illness or Infection?
Vitamin C is used rapidly during illness or infection because the body’s inflammatory response and metabolic demand surge simultaneously. According to a review published in Nutrients (MDPI), infections significantly impact vitamin C levels due to enhanced inflammation, and treatment of established infections requires gram doses of the vitamin to compensate for the increased metabolic demand. Fever, immune cell activation, and tissue repair all accelerate L-ascorbic acid consumption, often depleting plasma stores far faster than oral intake can replenish. This is precisely why intravenous delivery becomes valuable during acute illness; it restores plasma saturation quickly when the body’s antioxidant capacity is under the greatest strain.
How Fast Is Vitamin C Used Under Oxidative Stress?
Vitamin C is used at an accelerated rate under oxidative stress because it serves as a primary electron donor that neutralizes free radicals. When reactive oxygen species overwhelm the body’s antioxidant capacity, L-ascorbic acid is consumed rapidly to protect cells from damage. Conditions that increase oxidative burden, such as smoking, intense exercise, environmental toxin exposure, and chronic inflammation, deplete circulating vitamin C faster than baseline metabolic activity alone. Sodium ascorbate and other forms of vitamin C function similarly in scavenging free radicals, but once plasma stores drop, collagen synthesis and immune signaling also suffer. For individuals facing persistent oxidative stress, periodic IV vitamin C sessions can help maintain adequate plasma levels more effectively than oral supplementation.
How Fast Is Vitamin C Used Under Normal Conditions?
Vitamin C is used gradually under normal conditions, with the body drawing on circulating L-ascorbic acid for collagen synthesis, antioxidant maintenance, and routine enzymatic functions at a steady, manageable pace. Renal clearance returns elevated plasma levels to baseline within hours after an IV infusion, but tissue stores sustain functional levels longer when metabolic demand is low. As the Mayo Clinic notes, intravenous ascorbic acid should be used with caution in patients with kidney disease or a history of kidney stones, as it may worsen these conditions. For healthy individuals without these risk factors, the kidneys efficiently regulate vitamin C through the renal threshold, excreting excess while tissues retain what they need.
Understanding how quickly your body depletes IV vitamin C helps determine the ideal infusion frequency.
What Blood Levels Does IV Vitamin C Achieve Compared to Oral?
IV vitamin C achieves plasma concentrations up to 70 times higher than the maximum oral dose allows. This difference stems from how each route interacts with the body’s absorption controls.
Oral vitamin C faces tight intestinal regulation. According to pharmacokinetic studies cited by the National Cancer Institute, oral doses produce plasma concentrations capped below 300 μM because the gut limits how much enters the bloodstream. Doses above 500 mg see progressively less absorption as intake rises.
Intravenous vitamin C bypasses this intestinal control entirely, delivering L-ascorbic acid straight into the bloodstream. Plasma concentrations can reach up to 20 mM, a level impossible through oral supplementation alone. These supraphysiological concentrations are what make high-dose protocols relevant in clinical research settings.
However, the body does not sustain these elevated levels for long. Renal excretion begins rapidly once plasma saturation exceeds the renal threshold, restoring concentrations to baseline within hours. At doses up to 75 g, IV vitamin C follows first-order pharmacokinetics, meaning clearance rate scales proportionally with concentration.
For context, healthy young adults taking 200 to 400 mg orally per day typically reach steady-state plasma levels of only 60 to 80 μmol/L. That ceiling represents the body’s natural saturation point through dietary intake. The gap between 80 μmol/L orally and 20,000 μmol/L intravenously illustrates why route of administration matters so significantly for antioxidant capacity and therapeutic applications.
This concentration difference is worth understanding before deciding how frequently IV vitamin C infusions fit into a wellness routine.
How Often Should You Get IV Vitamin C Infusions?
IV vitamin C infusion frequency depends on your health goal. Immune support, post-surgical recovery, and general wellness each require different schedules based on how quickly your body depletes vitamin C.
How Often Should You Get IV Vitamin C for Immune Support?
You should get IV vitamin C for immune support every one to two weeks during periods of heightened exposure or seasonal illness. Infections significantly deplete vitamin C due to enhanced inflammation and increased metabolic demand, according to research published in Nutrients (MDPI). This accelerated turnover means the body exhausts its stores faster than oral supplementation alone can replenish them. During cold and flu season, or when traveling frequently, a biweekly schedule helps maintain elevated plasma levels. Once acute risk subsides, spacing sessions to monthly intervals is often sufficient to sustain baseline immune readiness.
How Often Should You Get IV Vitamin C for Recovery?
You should get IV vitamin C for recovery two to three times per week during the acute phase, then taper as healing progresses. Surgical and physical recovery creates substantial vitamin C depletion. A meta-analysis published in the British Journal of Nutrition found a mean plasma vitamin C depletion of 17.99 µmol/L, representing a 39% drop, during the first postoperative week. Because the body prioritizes vitamin C for collagen synthesis and tissue repair, frequent infusions during early recovery help maintain adequate plasma concentrations. As healing stabilizes over subsequent weeks, most individuals can reduce frequency to once weekly, then transition to a maintenance schedule. For athletes recovering from intense training cycles, a similar tapering approach supports tissue repair without oversaturation.
How Often Should You Get IV Vitamin C for General Wellness?
You should get IV vitamin C for general wellness once every two to four weeks. Healthy adults with balanced diets and low oxidative stress deplete vitamin C at a slower, more predictable rate. A monthly infusion typically sustains plasma levels well above the baseline range. Factors that may warrant more frequent sessions include:
Smoking, which lowers mean serum vitamin C by approximately one-third compared to non-smokers
High daily stress or poor dietary intake
Age-related absorption decline, particularly in adults over 65
For most wellness-focused clients, consistency matters more than frequency. A steady monthly schedule delivers cumulative antioxidant support without unnecessary visits. Understanding your personal depletion patterns helps determine the ideal schedule for sustained vitamin C benefits.
What Are the Signs That IV Vitamin C Has Left Your System?
The signs that IV vitamin C has left your system include a gradual return of fatigue, reduced energy levels, increased susceptibility to minor infections, and slower recovery from physical exertion. Because renal excretion restores vitamin C to baseline plasma concentrations within a few hours of intravenous administration, according to Oregon State University’s Linus Pauling Institute, these shifts can begin relatively quickly after peak levels decline.
Other indicators that your body’s elevated vitamin C stores have been depleted include:
Diminished skin brightness or increased dryness, since vitamin C supports collagen synthesis.
More pronounced muscle soreness after workouts, reflecting reduced antioxidant capacity.
Longer healing times for minor cuts or bruises.
A general feeling of sluggishness or brain fog that was absent shortly after infusion.
These signs do not necessarily mean you are deficient in vitamin C. They reflect the difference between the supraphysiological plasma concentrations achieved through IV delivery and your body’s normal baseline levels. Once the kidneys clear the excess ascorbic acid, plasma saturation drops back to its tightly regulated range, and the enhanced effects gradually fade.
Paying attention to when these subtle changes appear can help guide the timing of your next infusion session. Understanding how your body signals declining vitamin C levels makes it easier to maintain consistent wellness benefits over time.
Are There Side Effects of High-Dose IV Vitamin C?
The side effects of high-dose IV vitamin C are generally mild for most people, but certain individuals face serious risks. Key concerns include kidney-related complications and red blood cell damage in specific populations.
According to the Mayo Clinic, intravenous ascorbic acid injection may cause hemolysis, the breakdown of red blood cells, in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency. High-dose IV vitamin C should also be used with caution in patients with kidney disease or a history of kidney stones, as it may worsen these conditions.
Signs of a potential adverse reaction include:
Bloody urine or changes in urine output.
Lower back or side pain.
Unusual tiredness or weakness.
Decreased frequency or amount of urination.
G6PD deficiency testing before administration is considered a necessary screening step for anyone pursuing high-dose protocols. This simple blood test helps providers identify patients at risk for hemolysis before infusion begins.
For the majority of recipients without these contraindications, clinical trials have shown IV vitamin C to be generally well tolerated. That said, any high-dose therapy warrants professional oversight; even a well-tolerated infusion carries individual variability that only a qualified provider can properly assess. Understanding who should avoid this therapy entirely adds another layer of safety.
Who Should Avoid IV Vitamin C Therapy?
Individuals with specific medical conditions should avoid IV vitamin C therapy or use it only under strict medical supervision. The primary contraindications involve enzyme deficiencies, kidney disorders, and certain metabolic conditions.
People who should avoid or use caution with IV vitamin C include:
Individuals with G6PD deficiency: According to the Mayo Clinic, intravenous ascorbic acid injection may cause hemolysis, the breakdown of red blood cells, in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency. G6PD screening is considered essential before high-dose administration.
Patients with kidney disease or a history of kidney stones: IV vitamin C should be used with caution in these populations, as it may worsen existing renal conditions.
People experiencing warning signs such as bloody urine, decreased urination, lower back or side pain, or unusual fatigue: These symptoms may indicate a kidney problem requiring immediate medical attention.
For anyone considering high-dose IV vitamin C, pre-treatment screening and a thorough medical history review help identify these risk factors before infusion begins. Understanding contraindications is just as important as understanding how mobile IV services can deliver vitamin C safely and conveniently.
How Can Mobile IV Therapy Maximize Your Vitamin C Benefits?
Mobile IV therapy maximizes vitamin C benefits by delivering infusions directly to your location, eliminating delays between treatment and rest. The following subsections cover how The Drip IV Infusion supports immune health and the key takeaways about IV vitamin C duration.
Can The Drip IV Infusion’s Immune Support Infusions Help?
Yes. The Drip IV Infusion’s immune support infusions can help by delivering vitamin C and other nutrients intravenously, bypassing GI tract absorption limits for maximum bioavailability. Founded in Fall 2022 by professionals with decades of experience in nursing and emergency medicine, The Drip IV Infusion brings these treatments directly to homes and workplaces across Arizona. Each session takes approximately one hour and can be customized with add-ons like zinc, glutathione, and B-complex vitamins to complement the vitamin C infusion. This combination of convenience and clinical expertise makes it practical to maintain consistent vitamin C levels, especially for those recovering from illness or seeking immune support during high-demand periods.
What Should You Remember About How Long IV Vitamin C Stays in Your System?
The most important thing to remember about how long IV vitamin C stays in your system is that elevated plasma levels are temporary, typically returning to baseline within hours as the kidneys restore normal concentrations. Key takeaways include:
IV administration bypasses intestinal absorption limits, achieving plasma levels far beyond what oral doses allow.
Factors like kidney function, metabolic rate, illness, and hydration status all influence how quickly your body clears vitamin C.
Populations under higher oxidative stress, including smokers, older adults, and post-surgical patients, deplete vitamin C faster.
Consistent infusion scheduling, guided by a qualified nurse, helps maintain therapeutic benefits over time.
For most people, planning infusions based on individual health needs and lifestyle demands yields the best results. The Drip IV Infusion can help design a personalized schedule that keeps your vitamin C levels optimized between sessions.
If you’re curious about Normal Saline because you’ve heard about IV therapy or seen it mentioned when you’re at the doctor’s, you’re in the right place to learn everything about this basic medical solution. We get that you might be thinking about IV therapy or just want to know what’s going into your body during medical treatments. We’ll give you the straight facts you need to make smart choices.
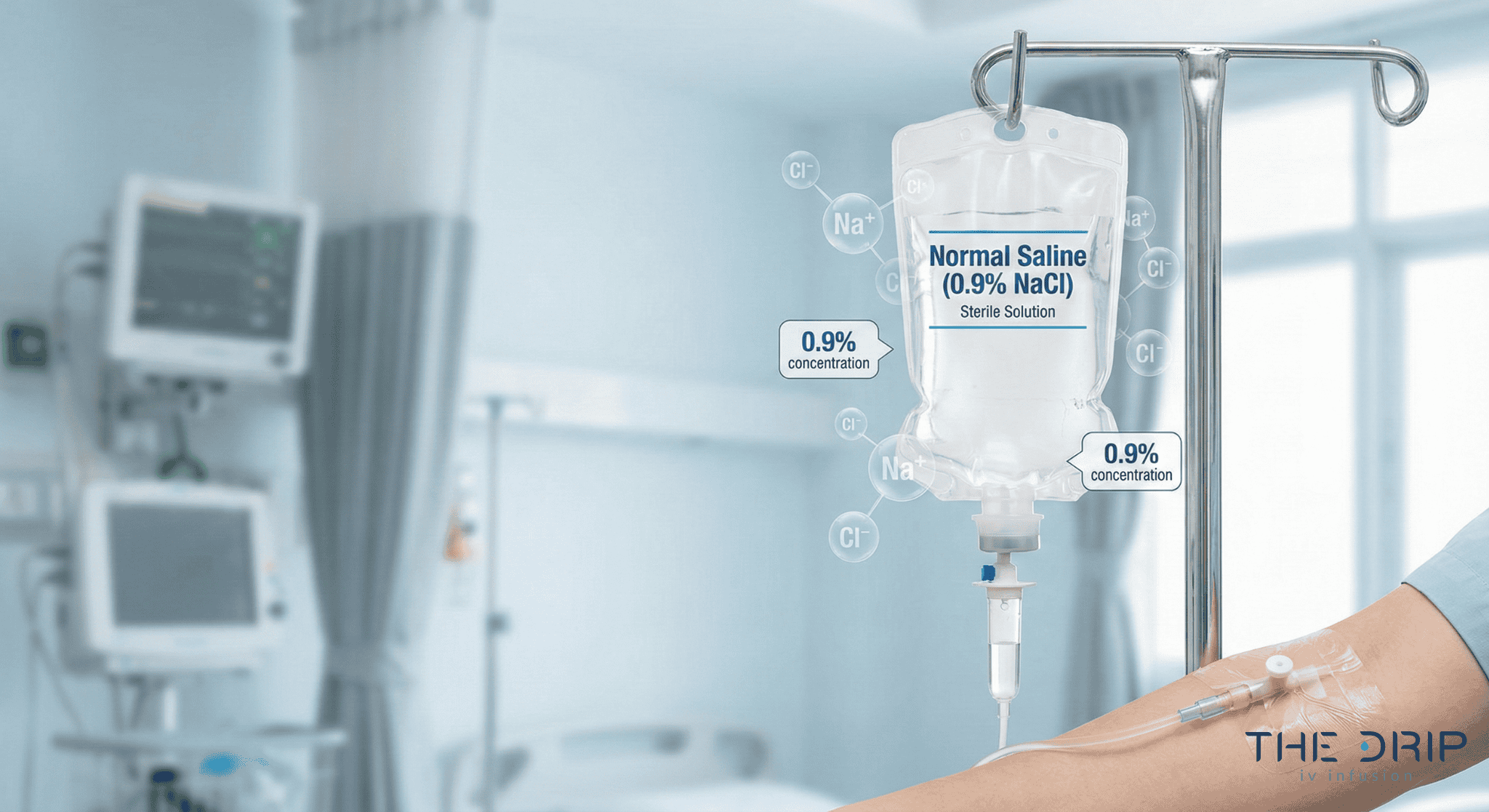
Normal Saline is a clean solution with 0.9% salt water that doctors use more than any other IV fluid around the world. This clear liquid has 9 grams of salt per liter – think of it like the salt content in your tears or sweat. Despite the name making it sound “normal” for your body, that’s actually a mix-up from way back in the 1800s when scientists got it wrong about what matched your blood.
New studies show other IV fluids might be safer for many people, though Normal Saline is still the best choice for brain injuries and certain conditions
Big amounts of Normal Saline can mess with your body’s acid balance and hurt your kidneys a bit more than other solutions
It only costs $1-2 to make but hospitals charge $127-700, making it the cheapest IV option
Doctors now pick IV fluids based on what you specifically need instead of just using Normal Saline for everyone
The Drip IV Infusion uses Normal Saline as a base for custom IV treatments, mixing its proven safety with extra nutrients
Quick Tip: If you’re getting an IV, ask your provider why they picked Normal Saline over other fluids – the answer should be about your specific health needs, not just because that’s what they always use.
What Are the Main Ingredients and Concentration of Normal Saline?
The main ingredients and concentration of Normal Saline are 0.9 grams of salt per 100 milliliters of water. This sterile solution contains specific amounts of sodium and chloride ions per liter, with a concentration slightly higher than your blood. The acidity level is higher than human blood. Understanding these specifications helps medical professionals and patients recognize why Normal Saline functions as a critical IV fluid in healthcare settings.
How Is Normal Saline Formulated?
Normal Saline is made by dissolving 9 grams of salt in one liter of sterile water. Each liter delivers specific amounts of sodium ions and chloride ions to your bloodstream. The solution maintains a concentration slightly higher than human blood.
Drug manufacturers produce Normal Saline as a clear, colorless, safe solution. The acidity typically measures around a level that’s more acidic than blood’s normal range. Production follows strict drug standards to ensure cleanliness and consistency.
The making process requires precise measurement and mixing under controlled conditions. Quality control tests verify the concentration, cleanliness, and absence of particles before distribution. These manufacturing standards ensure Normal Saline’s reliability as a medical-grade IV solution ready for immediate clinical use.
Why Is 0.9% Sodium Chloride Considered “Normal” Saline?
The 0.9% concentration is considered “Normal” Saline due to a historical misunderstanding from the 1800s. Scientists then incorrectly believed this concentration was perfectly balanced with mammalian blood. Dutch scientist Hartog Jakob Hamburger promoted the 0.9% standard in the late 1800s based on incomplete understanding of blood chemistry.
A 2016 study reveals that “the implied normalcy and physiological property have perpetuated indiscriminate use of saline in medical practice.” The term persists despite modern knowledge showing the solution’s chloride content exceeds normal levels. Dr. Thomas Latta first used IV saline during the 1831-1832 European cholera pandemic, establishing its medical foundation.
Today’s medical community recognizes Normal Saline as neither truly “normal” nor perfectly natural for your body. The name endures through medical tradition rather than scientific accuracy. This historical context explains why healthcare providers increasingly evaluate other fluid solutions for specific clinical scenarios where Normal Saline’s makeup may not be optimal.
How Is Normal Saline Used in Medical and Wellness Settings?
Normal Saline serves critical roles across medical and wellness applications. Healthcare providers use this 0.9% salt solution for fluid replacement, medicine delivery, and surgical support in diverse clinical scenarios.
In What Medical Situations Is Normal Saline Administered?
Medical situations for Normal Saline use include approved uses for replacing lost body fluid in dehydration, low blood volume, bleeding, and serious infections. The solution treats certain chemical imbalances when fluid loss occurs and manages mild sodium loss effectively.
Healthcare facilities use Normal Saline as a priming solution for kidney dialysis procedures. Medical teams use it to start and end blood transfusions safely. The solution works as a medicine mixer for compatible drug additives, enabling precise medication delivery.
Surgical teams apply Normal Saline as a washing solution during procedures to keep tissue moist and clear surgical fields. Emergency departments give it for acute adrenal problems, where rapid sodium replacement proves essential.
What Role Does Normal Saline Play in IV Therapy?
The role of Normal Saline in IV therapy centers on expanding blood volume through sodium and chloride ions. These primary chemicals of body fluid restore blood volume and maintain cell function.
Over 200 million liters of Normal Saline are used annually in the United States alone. The solution serves as the most widely used IV fluid in clinical practice worldwide. Healthcare providers rely on it as a vehicle for medicine delivery when working as a drug mixer.
Normal Saline enables rapid blood vessel access for emergency interventions. Medical teams select it for initial treatment before lab results become available.
How Is Normal Saline Used in Dehydration and Fluid Replacement?
Normal Saline is used in dehydration and fluid replacement by quickly restoring blood volume and correcting salt and water losses. The solution replaces lost fluids through vomiting, diarrhea, or excessive sweating.
Medical guidelines emphasize early, aggressive fluid replacement, though recent evidence favors more careful use. Clinical protocols now recommend careful volume assessment to prevent fluid overload complications.
Stomach doctors recommend against Normal Saline for acute pancreas inflammation, citing acid balance risk. Healthcare providers monitor acid-base balance during high-volume infusions to detect early signs of acid problems.
This widespread medical application of Normal Saline demonstrates its fundamental importance in healthcare delivery, though evolving evidence guides more selective use based on specific patient conditions.
What Are the Benefits and Limitations of Normal Saline?
Normal Saline offers distinct advantages and limitations that guide clinical decision-making in IV therapy. Healthcare providers weigh these factors when selecting fluids for specific patient needs.
What Are the Primary Advantages of Using Normal Saline?
Normal Saline provides several advantages in specific clinical scenarios where fluid balance is critical. These strengths make it one of the most frequently used solutions worldwide.
Key advantages include:
Safety for brain injury patients
Effective potassium reduction
Extremely low manufacturing cost
Simple single-chemical formulation
Broad medication and blood product compatibility
Are There Risks or Side Effects Associated with Normal Saline?
Yes. Normal Saline carries risks such as acid–base disturbances, kidney injury, fluid overload, and incompatibility with certain medicinesLarge-volume infusions cause acid balance problems due to high chloride concentration compared to what’s normally in your blood.
The SMART trial found Normal Saline associated with higher acute kidney injury rates compared to other fluids. Patients with heart or kidney problems face increased fluid overload risk. Normal Saline proves incompatible with certain medicines.
Situations where Normal Saline can’t be used include:
Significantly high sodium
High chloride
Significant fluid overload
Severe heart failure
Advanced kidney disease
When Might Alternative IV Solutions Be Preferred Over Normal Saline?
Other IV solutions are preferred over Normal Saline in serious infections, diabetic emergencies, pancreas inflammation, and severe liver disease. The SMART trial analysis showed other fluids reduced 30-day hospital deaths in infection patients compared to saline.Stomach doctors recommend other solutions over Normal Saline for pancreas inflammation.Choosing the right IV fluid depends on the clinical condition, acid–base effects, and metabolic capacity. The following table summarizes when alternatives outperform Normal Saline.
Clinical Scenario
Preferred Solution
Rationale
Sepsis
Balanced crystalloids
Lower mortality (SMART trial)
Diabetic ketoacidosis
Balanced crystalloids
Faster resolution
Acute pancreatitis
Lactated Ringer’s
Reduced metabolic acidosis risk
Severe liver disease
Normal Saline
Avoids lactate accumulation
Patients with severe liver disease benefit from Normal Saline over Lactated Ringer’s due to reduced lactate metabolism capacity. These clinical nuances inform individualized fluid selection strategies.
How Does Normal Saline Compare to Other IV Fluids?
Normal Saline compares to other IV fluids through distinct chemical makeups, acid levels, and clinical applications. The primary differences center on sodium and chloride concentrations versus balanced solutions containing additional chemicals. Understanding these comparisons helps medical providers select optimal fluid therapy based on patient conditions and treatment goals.
What Are the Key Differences Between Normal Saline and Lactated Ringer’s?
The key differences between Normal Saline and Lactated Ringer’s are found in their sodium, chloride, potassium, calcium, and lactate content. Normal Saline contains equal amounts of sodium and chloride, while Lactated Ringer’s contains less sodium and chloride.
Lactated Ringer’s includes additional chemicals absent in Normal Saline: • Potassium • Calcium • Lactate (turned into bicarbonate by your liver)
These makeup differences influence fluid distribution and body effects, making each solution suited for specific clinical scenarios.Normal Saline and Lactated Ringer’s differ significantly in electrolyte composition and physiologic effects. The table below highlights the main distinctions.
Solution
Sodium
Chloride
Additional Components
Acidity
Normal Saline
High
High
None
More acidic
Lactated Ringer’s
Moderate
Moderate
Potassium, Calcium, Lactate
Less acidic
Why Might a Medical Provider Choose Normal Saline Over Other Solutions?
A medical provider may choose Normal Saline over other solutions because it is safer for brain injury, better tolerated in liver disease, and more cost-effective. The BaSICS trial found higher death rates in brain injury patients treated with balanced solutions, reinforcing Normal Saline use for brain injury cases.
Normal Saline is preferred in liver disease patients because liver dysfunction may mess up chemical processing from other solutions, potentially raising chemical levels. Money considerations also influence selection – other fluids cost 2 to 4.5 times more than Normal Saline at wholesale level, creating pressure favoring Normal Saline use.
A 2025 major hospital study involving 43,000 patients found no significant difference in death or readmission between different fluid policies. This finding suggests both fluids provide comparable outcomes in general hospital populations.
These comparisons demonstrate that Normal Saline remains valuable for specific conditions despite the availability of other alternatives, with selection depending on individual patient factors and hospital protocols.
What Should Patients Know Before Receiving Normal Saline?
Normal saline administration requires careful patient assessment and monitoring. Healthcare providers evaluate specific medical conditions, situations where it can’t be used, and expected outcomes before starting therapy. Understanding who’s a good candidate, precautions, and infusion procedures helps patients make informed decisions about their treatment.
Who Is a Candidate for Normal Saline Infusion?
Candidates for Normal Saline infusion are patients who require rapid fluid replacement, sodium correction, dialysis priming, or brain-injury-appropriate fluids. There are four primary indications: volume loss states such as dehydration and low blood volume, chemical imbalances including certain alkaline conditions, procedural requirements for dialysis priming, and brain conditions like traumatic brain injury.
Patients experiencing significant blood loss benefit from normal saline’s rapid volume expansion properties. Those with mild sodium loss receive targeted chemical replacement through the solution’s sodium content. Healthcare providers select normal saline for brain-injured patients because proper fluids prevent brain swelling from worsening.
The following sections detail specific precautions and monitoring requirements for these patient populations.
What Precautions or Contraindications Exist for Normal Saline?
Clinicians must screen patients for conditions that worsen with excess sodium or chloride.
Normal Saline should NOT be used in patients with: ☐ High sodium ☐ High chloride ☐ Lung fluid buildup ☐ Significant fluid overload ☐ Sodium-sensitive cardiac or renal conditions
Monitoring protocols help identify complications early during treatment.
What Can Patients Expect During a Normal Saline Infusion?
Patients can expect close monitoring of urine output, swelling, vital signs, and lab values during a Normal Saline infusion. Healthcare teams track urine output targeting above specific levels and assess for swelling development. Lab monitoring includes blood chemicals, bicarbonate, kidney function tests, and blood gases.
Critically ill patients receive advanced monitoring through central line pressure measurements and heart ultrasound assessments. Despite production costs of $1-2 per liter, hospital charges range from $127 to over $700 per bag.
A team coordinates care delivery. Doctors prescribe appropriate volumes, nurses monitor vital signs and infusion rates, and pharmacists verify medicine compatibility. This team approach ensures safe administration while detecting adverse effects promptly.
Understanding these aspects of normal saline therapy prepares patients for their treatment experience and promotes informed participation in care decisions.
How Can You Safely Experience the Benefits of Normal Saline IV Therapy with The Drip IV Infusion?
Normal Saline IV therapy offers rapid hydration and chemical balance when given by qualified professionals. The Drip IV Infusion ensures safe delivery through medical oversight, clean protocols, and personalized treatment plans tailored to individual wellness needs.
How Does The Drip IV Infusion Incorporate Normal Saline in Its Services?
The Drip IV Infusion incorporates Normal Saline as the foundation of its customized IV therapy treatments. Each infusion begins with drug-grade 0.9% salt solution meeting strict cleanliness standards. Licensed medical professionals assess hydration status before determining appropriate volume and infusion rate.
The Drip IV Infusion combines Normal Saline with vitamins, minerals, and antioxidants based on specific wellness goals. Treatment options include hydration therapy, athletic recovery, immune support, and energy enhancement formulas. Mobile service brings treatments directly to homes, offices, or hotels for convenience.
Medical screening protocols ensure safety before each infusion. Nurses monitor vital signs throughout treatment and adjust flow rates as needed. The Drip IV Infusion maintains emergency protocols and supplies for immediate response to any bad reactions.
What Are the Key Takeaways About What Is Normal Saline?
The key takeaways about Normal Saline are that it is a 0.9% salt solution with proven safety, specific advantages, and growing competition from alternative fluids. Normal Saline contains 0.9% salt, providing specific amounts of sodium and chloride ions per liter. This solution expands blood volume without causing harmful fluid shifts.
A 2025 major trial involving 43,000 patients found no significant death difference between Normal Saline and other fluids in general hospital populations. The BaSICS trial confirmed Normal Saline superiority for brain injury patients. Manufacturing costs remain low at $1-2 per liter, though hospital charges range from $127-700.
Recent evidence supports individualized fluid selection rather than universal protocols. The SMART trial showed other fluids reduced kidney injury rates compared to Normal Saline. Medical experts advocate careful clinical reasoning when selecting IV fluids based on patient-specific factors.
The Drip IV Infusion applies this evidence-based approach through comprehensive assessment and customized treatment protocols, ensuring clients receive appropriate IV therapy aligned with current medical guidelines and individual wellness objectives.
IV hydration therapy is an effective way to get the necessary nutrients and vitamins into your body. Due to the practical way of application, this type of IV therapy offers numerous benefits and advantages compared to other ways of administration. So, what IV hydration therapy benefits should you know before deciding on this type of therapy?
Stay with us as we analyze the benefits of IV hydration therapy. In addition, we will provide you with useful tips to help you choose IV therapy according to your health needs.
6 Amazing IV Hydration Therapy Benefits
Initially, intravenous therapy was administered in healthcare facilities to patients with nutrient deficiencies, dehydration, or patients who were unable to take medications orally. Today, IV therapy is quite popular, even among healthy individuals who want to increase their energy levels and well-being.
In addition to health facilities that administer this therapy, you can get at home IV therapy service in Queen Creek. Also, there are numerous IV hydration therapy benefits that you should consider. In the following, we will look at some of the most important advantages offered by this therapy:
As the name suggests, one of the main benefits of IV hydration therapy is rapid rehydration. Whether it is due to hard work, physical activity, or a medical condition, the body can lose the necessary nutrients and lead to dehydration.
Before IV hydration therapy became popular, drinking water was considered the best solution for dehydration. However, most of this water is absorbed in the digestive system and not the rest of the body.
To allow easier absorption of nutrients, many opt for IV hydration therapy. Through this therapy, nutrients are administered directly through the bloodstream, bypassing the digestive system, which may be an effective way to hydrate those parts of the body that need it most.
Enhanced absorption and effectiveness
In addition to rehydration, IV therapy offers a high degree of absorption and utilization of nutrients. Namely, when vitamins, minerals, and nutrients are taken orally, the body absorbs only a part while a large part passes through the digestive system.
Unlike oral intake of nutrients, using IV hydration therapy allows a 90-100% absorption of nutrients for optimal use and minimal waste. By administering IV fluids, the vitamins and minerals are delivered directly to the cells that need them.
Improved energy levels and performance
IV hydration therapy may help physically active people, especially athletes. Through increased physical exertion during training or competition, athletes may experience loss of fluids.
This therapy allows faster hydration and recovery to athletes after hard training. In addition, IV hydration therapy contains important elements such as fluids, electrolytes, vitamins, and minerals that may raise energy levels and help improve focus.
Immunity enhancement
Due to effective administration, IV therapy may help improve immunity. The ingredients in this therapy, like Vitamin C and Vitamin B12, may help fight various infections and increase energy in the body. Unlike oral intake, the ingredients from IV hydration therapy are introduced directly into the bloodstream, which allows them to reach those parts of the body where they are most needed.
Supports collagen production
Collagen is an essential element that can help smooth the skin, increase elasticity, and reduce wrinkles. With aging, collagen synthesis is reduced, and thus, the skin’s elasticity is lost.
Through IV drip hydration, the body may be supplied with the necessary vitamins and minerals to help slow the aging process and stimulate collagen production. Namely, this therapy may contain Vitamins C and Glutathione, which play an important role in collagen synthesis.
Vitamin C is a powerful antioxidant that may protect cells from deterioration and depletion. In addition, Vitamin C protects the skin from UV rays and is the main element against dry skin. Glutathione is also an antioxidant that may help slow down the aging process by controlling melanin synthesis.
Quick Relief from Symptoms
The ingredients in IV therapy may also help with more common symptoms such as nausea, fatigue, and even headache. Such conditions may occur due to a lack of fluid intake and lack of proper nutrition. Due to the direct intake of nutrients into the bloodstream, IV therapy may help with several conditions, such as:
Although IV hydration therapy may offer multiple benefits, you should pay attention to your needs and overall health. Namely, the choice of ingredients in IV therapy depends on several factors such as daily activities, diet, etc.
Before deciding on this type of therapy, it is important to consult with a healthcare professional to determine the type of IV therapy that will be most effective.
In addition to the type of IV therapy, you should emphasize with the healthcare professional whether you are allergic to any substance, medicine, or food. In addition, it is important to list all past illnesses and any prescribed medications you have. IV therapy should not be a substitute for prescribed medications from your doctor. If you are receiving regular prescribed therapy, consult with a healthcare professional about whether it is good to include IV therapy in your supplemental treatment plan.
Conclusion
IV therapy is a great way to get the necessary ingredients that can benefit your general well being. Since there are many IV hydration therapy benefits, it is important to discuss with a healthcare professional whether you are an ideal candidate for this type of therapy.
Vitamin B12 plays a vital role in many metabolic processes in the body. Although the human body cannot produce this vitamin, it is consumed through food such as meat and dairy products. So, what are B12 IV benefits?
Continue reading to learn in detail about the benefits of intravenous therapy and vitamin B12.
The main benefit of B12 IV is how it is administered. Specifically, intravenous administration bypasses the digestive system, delivering nutrients directly into the bloodstream. This way, you may quickly get all the advantages of the administered IV fluid.
You can receive this type of therapy at a health facility, or you can get it at home IV therapy service in Queen Creek. In addition to the method of administration, B12 IV therapy may help with several health conditions. We explained them in the following.
Energy boost and metabolism
One of the important B12 IV drip benefits might be improved concentration and energy levels. In other words, B12 is necessary to produce red blood cells that transport oxygen and nutrients throughout the body. Thus, by increasing oxygen in the bloodstream, vitamin B12 may help improve cognitive function and increase energy levels in the body.
Cardiovascular health
An amino acid called homocysteine is produced by breaking down proteins in the body. This amino acid, when produced in large amounts, may be the cause of many heart diseases.
Also, an increased level of homocysteine may be the result of an unregulated diet and bad habits such as alcohol or coffee. By taking in B12, the homocysteine level may be reduced, potentially lowering the chances of cardiovascular diseases.
Skin, hair, and nail improvement
B12 plays a role in hair, nails, and skin health due to its role in cell production. However, lacking this vitamin may lead to dry and brittle hair, discolored nails, cracked mouth corners, etc.
Mood improvement and mental health
Besides the above-mentioned B12 IV infusion benefits, it may help with enhancing mood. Additionally, the B complex vitamins—B12 in particular—may be quite important for maintaining brain function.
This vitamin is important for serotonin metabolism, a chemical key to your mood. Reduced blood B12 levels lead to decreased serotonin production and, consequently, reduced mood.
If the condition persists, it may lead to more severe forms of depression. Therefore, by supplementing B12 levels within normal limits, mood may be elevated, and certain negative health conditions may be avoided.
Exercise performance and recovery
Vitamin B12 may help improve athletic performance and aid recovery after strenuous exercise. Some studies suggest that B12 may accomplish this function by ensuring the proper functioning of the central nervous system and the production of red blood cells that deliver oxygen to muscle tissue.
In addition, this vitamin may help produce fatty acids, proteins, and amino acids essential for muscle recovery after a hard workout. Hence, this therapy may help people who are actively involved in sports or need energy.
Hematological benefits
Intravenous B12 therapy may have hematological benefits as well. Such benefits relate to the prevention of anemia by the production of red blood cells. Anemia is when you don’t have healthy red blood cells capable of carrying oxygen to the tissues.
Such red blood cells in B12-deficient patients have a large oval shape and cannot move easily through the bloodstream. However, this condition of red blood cells may be improved with B12 IV therapy, and the cells can function optimally.
Source: thedripivinfusion.com
Things to Consider Before B12 IV Therapy
If your doctor has recommended IV therapy, there are a few things to consider. First, your healthcare provider should be thoroughly familiar with your medical condition.
For this purpose, you should emphasize if you are allergic to any ingredient found in the IV fluid. That way, the healthcare provider will prepare a combination of ingredients that match your health condition. In addition, you should list all past and present illnesses, including hereditary diseases.
If you are taking a prescribed therapy, list the name and how often you take it. Doing so reduces the risk of IV therapy ingredients reacting with regular therapy ingredients.
How Much Does IV Therapy Cost?
If you want to take B12 IV therapy, please note that this treatment has no specific price. First, the factors that affect the price are the composition of the IV fluids and the place where you receive this therapy. You can check the prices of our IV cocktails here.
Many insurance companies do not cover this type of IV therapy, so the cost will be out of pocket. This treatment is relatively safe and typically has an immediate impact on your overall wellness.
So, if your condition requires IV therapy, it is good to consult with your doctor or healthcare provider about the type of IV therapy, benefits, possible risks, and cost.
Conclusion
We hope it has become clearer to you about the B12 IV benefits. So, if you decide on this therapy, keep in mind that mobile IV therapy does not replace regular therapy prescribed by a doctor. You should always consult a healthcare professional to determine if you are an ideal candidate.