IV antibiotics are antimicrobial medications delivered directly into the bloodstream through a vein, bypassing the gastrointestinal tract to achieve 100% bioavailability and immediate therapeutic effect. Physicians prescribe them when infections are too severe, too deep, or too urgent for oral therapy to deliver adequate drug concentrations.
This guide covers the clinical rationale behind IV versus oral antibiotics, the most commonly prescribed IV antibiotic drugs, how they are administered and for how long, the conditions they treat, their side effects and risks, and how supportive IV therapy can complement recovery.
Some infections respond well to oral antibiotics, but conditions like sepsis, bacterial meningitis, endocarditis, and osteomyelitis often demand intravenous delivery because oral agents cannot maintain the sustained blood concentrations these infections require. Bioavailability differences between specific drugs determine when an IV-to-oral switch is clinically appropriate.
We cover eight major IV antibiotics, including vancomycin, ceftriaxone, piperacillin-tazobactam, and meropenem, each targeting different bacterial pathogens. Administration methods range from short-term peripheral IV lines to PICC lines and central venous catheters for extended treatment courses.
Treatment duration varies significantly by condition, from 7 days for some sepsis cases to 6 weeks for endocarditis. Side effects range from infusion site reactions to nephrotoxicity, allergic responses, and C. difficile infection, all of which require active monitoring.
For eligible patients, outpatient parenteral antibiotic therapy (OPAT) provides a cost-effective alternative to prolonged hospitalization. We also address antibiotic resistance, questions to ask your doctor, and how mobile IV hydration and immune support can complement prescribed treatment during recovery.
What Are IV Antibiotics?
IV antibiotics are antimicrobial medications delivered directly into the bloodstream through a vein. Unlike oral antibiotics that must pass through the digestive system, IV antibiotics bypass the gastrointestinal tract entirely. This delivers 100% bioavailability, meaning the full dose reaches the bloodstream immediately. Physicians prescribe IV antibiotics for serious or life-threatening infections where rapid, reliable drug concentrations are critical.
According to the National Library of Medicine, intravenous antibiotic therapy ensures immediate therapeutic effect by bypassing the gastrointestinal tract’s absorption barriers. This makes IV administration essential when patients cannot tolerate oral medications, when infections are too severe for oral treatment alone, or when specific drug levels must be precisely maintained in the blood.
Common scenarios requiring IV antibiotics include:
- Severe bacterial infections such as sepsis, meningitis, or endocarditis.
- Cases where patients experience vomiting, malabsorption, or inability to swallow.
- Infections caused by resistant organisms that require high sustained drug concentrations.
- Post-surgical infections needing rapid antimicrobial response.
IV antibiotics encompass several major drug classes, each targeting different bacterial organisms. These include beta-lactams like ceftriaxone and piperacillin-tazobactam, glycopeptides like vancomycin, carbapenems like meropenem, and nitroimidazoles like metronidazole. The choice depends on the infection type, bacterial susceptibility, and patient-specific factors.
For clinicians and patients alike, understanding when IV antibiotics are necessary versus when oral therapy suffices is a foundational decision in infection management. The sections below cover why IV antibiotics are chosen over oral options, the most common types prescribed, how they are administered, and what side effects to watch for.
Why Are IV Antibiotics Used Instead of Oral Antibiotics?
IV antibiotics are used instead of oral antibiotics when infections are too severe, too deep, or too urgent for the gastrointestinal tract to deliver adequate drug levels. The following subsections cover when oral therapy falls short, which infections demand IV delivery, and how bioavailability shapes that clinical decision.
When Is Oral Antibiotic Therapy Not Enough?
Oral antibiotic therapy is not enough when a patient cannot absorb medication through the gastrointestinal tract, when an infection requires immediate peak drug concentrations, or when the severity of illness demands guaranteed delivery. IV antibiotic therapy bypasses the GI tract entirely, ensuring 100% bioavailability and immediate therapeutic effect.
Clinical criteria for switching from IV to oral include clinical improvement, fever resolution, hemodynamic stability, and the ability to tolerate oral intake without malabsorption concerns. Notably, the assumption that IV always outperforms oral is increasingly challenged. According to Dr. Brad Spellberg, an infectious disease specialist writing in Open Forum Infectious Diseases, “no prospective study ever established IV antimicrobial therapy as more effective than oral therapy for the treatment of osteomyelitis or endocarditis.” The IDSA 2021 guidelines for pediatric osteomyelitis similarly recommend a short IV course followed by oral transition, finding outcomes comparable to prolonged IV therapy.
What Types of Infections Require IV Antibiotics?
The types of infections that require IV antibiotics are generally those involving deep tissue, the bloodstream, or critical organs where rapid, sustained drug levels are essential. These include:
- Sepsis and bloodstream infections requiring immediate antimicrobial action
- Bacterial meningitis, where antibiotics must cross the blood-brain barrier at high concentrations
- Infective endocarditis involving heart valve tissue
- Osteomyelitis during the initial stabilization phase
- Severe pneumonia unresponsive to oral therapy
- Complicated intra-abdominal and urinary tract infections
According to a study published in the National Library of Medicine, time-dependent antibiotics like beta-lactams require drug concentrations above the minimum inhibitory concentration for 40% to 50% of the dosing interval, and continuous IV infusions are associated with reduced hospital stays and mortality. For many of these conditions, oral agents simply cannot maintain those thresholds reliably enough during the critical window.
How Does Bioavailability Differ Between IV and Oral Antibiotics?
Bioavailability differs between IV and oral antibiotics primarily in absorption consistency. IV administration delivers 100% of the drug directly into the bloodstream, while oral bioavailability varies widely depending on the specific antibiotic and the patient’s GI function.
According to a review published in the National Library of Medicine, antibiotics like metronidazole and fluconazole achieve oral bioavailability exceeding 90%, making them strong candidates for an IV-to-oral switch once a patient is clinically stable and tolerating intake. Other drugs, particularly certain beta-lactams and aminoglycosides, have significantly lower oral absorption, which is why they remain IV-only options. This bioavailability gap is the core pharmacological reason clinicians choose IV delivery for acute, life-threatening infections where guaranteed drug levels are non-negotiable.
With the clinical rationale for IV antibiotics established, the next section covers the specific drug classes most commonly administered intravenously.
What Are the Common Types of IV Antibiotics?
The common types of IV antibiotics include vancomycin, ceftriaxone, piperacillin-tazobactam, meropenem, metronidazole, ampicillin-sulbactam, cefazolin, and daptomycin. Each targets different bacterial pathogens and infection types.
Vancomycin
Vancomycin is a glycopeptide antibiotic used primarily against gram-positive bacteria, including methicillin-resistant Staphylococcus aureus (MRSA). Clinicians rely on it for serious infections such as bacteremia, endocarditis, osteomyelitis, and complicated skin infections where resistant organisms are suspected. Because vancomycin requires careful dose monitoring to maintain therapeutic trough levels, patients typically undergo regular blood draws during treatment. Infusion rate also matters; administering it too quickly increases the risk of adverse reactions. For most practitioners, vancomycin remains an indispensable first-line option when MRSA coverage is needed, though rising minimum inhibitory concentrations in some Staphylococcus aureus isolates warrant ongoing vigilance.
Ceftriaxone
Ceftriaxone is a third-generation cephalosporin with broad gram-negative coverage and convenient once-daily dosing. According to the Johns Hopkins ABX Guide, ceftriaxone is typically dosed at 1 to 2 grams daily, with a maximum of 4 grams for meningitis, and resistance frequently emerges via AmpC induction or extended-spectrum beta-lactamase (ESBL) production. Common indications include bacterial meningitis, community-acquired pneumonia, urinary tract infections, and Lyme disease. Its long half-life makes ceftriaxone particularly practical for outpatient parenteral antibiotic therapy, where fewer daily infusions improve patient compliance and quality of life.
Piperacillin-Tazobactam
Piperacillin-tazobactam is a broad-spectrum penicillin and beta-lactamase inhibitor combination effective against many gram-negative, gram-positive, and anaerobic bacteria. According to the Infectious Diseases Society of America, piperacillin-tazobactam is commonly dosed at 4.5 grams every 6 to 8 hours, often via extended 3- to 4-hour infusions to optimize pharmacodynamics against Pseudomonas aeruginosa. Clinicians frequently prescribe it for intra-abdominal infections, hospital-acquired pneumonia, and complicated skin infections. Extended infusion protocols represent one of the most effective strategies for maximizing this antibiotic’s time-dependent killing activity.
Meropenem
Meropenem is a carbapenem antibiotic reserved for severe or multidrug-resistant infections. It provides exceptionally broad coverage against gram-negative, gram-positive, and anaerobic organisms. The IDSA recommends carbapenems like meropenem as the preferred treatment for serious infections caused by ESBL-producing Enterobacterales, due to concerns about the inoculum effect and inferior clinical outcomes with alternatives in bloodstream infections. Common uses include complicated intra-abdominal infections, bacterial meningitis, and febrile neutropenia. Because carbapenems are considered “last-resort” agents, responsible stewardship practices are essential to preserve their effectiveness.
Metronidazole
Metronidazole is an antibiotic that targets anaerobic bacteria and certain parasitic organisms. According to a study published in Antimicrobial Agents and Chemotherapy, metronidazole maintained near 100% susceptibility against Bacteroides species, while ampicillin-sulbactam and clindamycin showed decreasing susceptibility over time. Physicians commonly prescribe it for intra-abdominal infections, Clostridioides difficile colitis, brain abscesses, and pelvic infections. Notably, metronidazole has oral bioavailability exceeding 90%, which often makes it a strong candidate for early IV-to-oral switch therapy once patients demonstrate clinical improvement.
Ampicillin-Sulbactam
Ampicillin-sulbactam is a penicillin and beta-lactamase inhibitor combination that covers many gram-positive, gram-negative, and anaerobic pathogens. Clinicians use it frequently for community-acquired intra-abdominal infections, gynecologic infections, aspiration pneumonia, and diabetic foot infections. The sulbactam component restores activity against beta-lactamase-producing organisms that would otherwise resist ampicillin alone. While its anaerobic susceptibility profile has declined compared to metronidazole, ampicillin-sulbactam remains a practical empiric choice for mixed polymicrobial infections where broad but not ultra-wide coverage is appropriate.
Cefazolin
Cefazolin is a first-generation cephalosporin with strong gram-positive coverage and a well-established safety profile. It serves as the standard choice for surgical prophylaxis across orthopedic, cardiac, and abdominal procedures. Cefazolin also treats methicillin-susceptible Staphylococcus aureus (MSSA) bacteremia, skin and soft tissue infections, and uncomplicated urinary tract infections. Its predictable pharmacokinetics, infrequent dosing schedule, and low cost make it one of the most widely administered IV antibiotics in both inpatient and outpatient settings.
Daptomycin
Daptomycin is a cyclic lipopeptide antibiotic active against gram-positive organisms, including MRSA and vancomycin-resistant enterococci (VRE). It works by disrupting the bacterial cell membrane, causing rapid depolarization and cell death. Clinicians prescribe daptomycin for complicated skin infections, bacteremia, and right-sided endocarditis. One critical limitation is that daptomycin cannot treat pneumonia because pulmonary surfactant inactivates the drug. For patients who fail vancomycin therapy or have vancomycin-resistant infections, daptomycin provides an essential alternative.
Understanding each antibiotic’s spectrum and clinical role helps guide appropriate therapy decisions.
How Are IV Antibiotics Administered?
IV antibiotics are administered through three primary vascular access methods: peripheral IV lines, PICC lines, and central venous catheters. Each method suits different treatment durations and clinical needs.
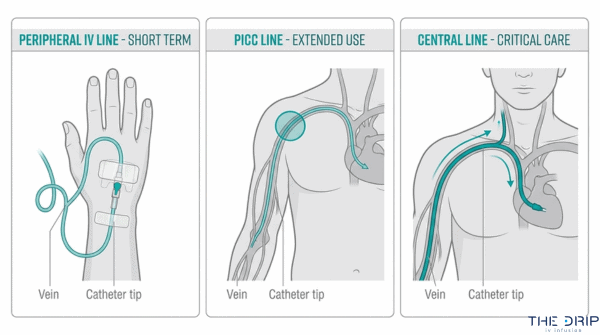
What Is Peripheral IV Antibiotic Administration?
Peripheral IV antibiotic administration is the delivery of antibiotics through a short catheter inserted into a small vein, typically in the hand or forearm. A healthcare provider places the catheter using a small needle, then secures it with adhesive dressing. This method works best for short-term treatments lasting a few days, since the catheter usually requires replacement every 72 to 96 hours to reduce infection risk. Peripheral lines are the most common starting point for IV antibiotics in emergency rooms and hospitals because insertion is quick and minimally invasive. However, certain medications that irritate smaller veins may require a larger central line instead.
What Is a PICC Line for IV Antibiotics?
A PICC line for IV antibiotics is a long, flexible catheter inserted into a vein in the upper arm and threaded until the tip rests near the heart. This positioning allows delivery of medications that would damage smaller peripheral veins. PICC lines can remain in place for weeks to months, making them ideal for extended antibiotic courses such as those required for osteomyelitis or endocarditis. A trained nurse or interventional radiologist typically places the line using ultrasound guidance. Because PICC lines are durable and reliable for long-term outpatient use, they are the most frequently chosen access device for home IV antibiotic therapy.
What Is a Central Venous Catheter for IV Antibiotics?
A central venous catheter (CVC) for IV antibiotics is a large-bore catheter placed directly into a major vein, usually the internal jugular, subclavian, or femoral vein. CVCs enable rapid delivery of high-volume fluids and multiple medications simultaneously, which makes them essential in critical care settings. Surgically implanted ports represent another CVC option for patients requiring intermittent long-term access. According to a study published in the National Library of Medicine, PICC-related bloodstream infection rates reached 14.38 per 1,000 catheter-days in hospitalized patients compared to 3.19 per 1,000 catheter-days in outpatients. This highlights why infection prevention protocols, including sterile dressing changes and regular site assessment, are critical for any central line.
How Long Does a Typical IV Antibiotic Infusion Take?
A typical IV antibiotic infusion takes between 15 minutes and 4 hours, depending on the specific drug and dosing protocol. Rapid infusions of antibiotics like ceftriaxone often complete within 30 minutes. Vancomycin, by contrast, requires slower administration over at least 60 minutes to reduce the risk of adverse reactions. Some beta-lactam antibiotics benefit from extended 3 to 4 hour infusions that maintain drug concentrations above effective levels for longer periods. Continuous 24-hour infusions are occasionally used in intensive care for critically ill patients. The prescribing physician determines the exact rate based on the medication, infection severity, and patient tolerance.
With administration methods in place, the next consideration is which conditions most commonly require IV antibiotics.
What Conditions Are Commonly Treated With IV Antibiotics?
The conditions commonly treated with IV antibiotics include sepsis, bacterial meningitis, endocarditis, osteomyelitis, severe pneumonia, complicated urinary tract infections, cellulitis, and intra-abdominal infections.
Sepsis and Bloodstream Infections
Sepsis and bloodstream infections require immediate IV antibiotic therapy to control rapidly spreading bacteria in the circulatory system. Early administration is critical because delays in treatment increase mortality risk significantly with each passing hour. According to IDSA guidance, for serious infections caused by ESBL-producing Enterobacterales, carbapenems like meropenem are preferred over piperacillin-tazobactam due to concerns about the inoculum effect and inferior clinical outcomes in bloodstream infections. Empiric broad-spectrum coverage is typically started before culture results return, then narrowed once the causative organism is identified.
Bacterial Meningitis
Bacterial meningitis is one of the most urgent conditions requiring IV antibiotics, with treatment often initiated within minutes of clinical suspicion. According to the World Health Organization, approximately 1 in 6 affected individuals die, while 1 in 5 suffer severe long-term complications; meningococcal-specific cases carry a 10% to 15% mortality rate even with treatment. High-dose IV cephalosporins penetrate the blood-brain barrier to reach therapeutic concentrations in cerebrospinal fluid. Adjunctive intravenous dexamethasone is also recommended to reduce neurological sequelae, though clinical trial results remain conflicting regarding its overall impact on mortality.
Endocarditis
Endocarditis requires prolonged IV antibiotic therapy because the infection affects heart valve tissue, which has limited blood supply. Biofilm formation on damaged valves makes bacterial eradication particularly difficult, often necessitating four to six weeks of continuous intravenous treatment. Combination regimens targeting the specific causative organism are standard, with agents selected based on blood culture sensitivity results.
Osteomyelitis
Osteomyelitis involves bacterial infection of bone tissue, where poor vascular supply limits oral drug penetration. IV antibiotics deliver high-concentration drug levels directly to the bloodstream, improving distribution to infected bone. Treatment typically begins with an IV course before transitioning to oral therapy once clinical improvement is confirmed, a strategy the IDSA supports as equally effective for most patients.
Severe Pneumonia
Severe pneumonia requires IV antibiotics when patients cannot absorb oral medications or when the infection has progressed to respiratory failure. According to the 2021 Global Burden of Disease report, severe pneumonia causes an estimated 2.1 million deaths annually, particularly among children under 5 and adults over 70. Treatment duration for severe cases typically averages 13.5 days. The combination of high mortality risk and compromised respiratory function makes intravenous administration essential for achieving rapid therapeutic drug levels.
Complicated Urinary Tract Infections
Complicated urinary tract infections involve structural abnormalities, catheter use, or resistant organisms that prevent standard oral therapy from resolving the infection. Clinical guidelines often favor a 14-day treatment duration for cUTIs, according to the American Journal of Kidney Diseases, although shorter 7-day courses are increasingly considered for patients showing rapid clinical response. This shift toward individualized treatment duration reflects growing emphasis on antibiotic stewardship without compromising outcomes.
Cellulitis and Severe Skin Infections
Cellulitis and severe skin infections warrant IV antibiotics when the infection spreads rapidly, involves deeper tissue layers, or fails to respond to oral therapy. Purulent infections with systemic signs, such as fever or elevated white blood cell counts, often require intravenous agents targeting both streptococcal and staphylococcal species. Patients with immunocompromising conditions face higher risk of progression, making early IV intervention particularly important.
Intra-Abdominal Infections
Intra-abdominal infections involve bacterial contamination of the peritoneal cavity from sources such as perforated appendicitis, diverticulitis, or post-surgical complications. According to a study published in the National Library of Medicine, complicated intra-abdominal infections carry an overall mortality rate of approximately 9.2%, exceeding 20% in critically ill patients who develop multiple organ dysfunction syndrome. Broad-spectrum IV regimens covering gram-negative, gram-positive, and anaerobic organisms are standard. Understanding which infections demand IV therapy helps clarify how long treatment typically lasts.
How Long Does IV Antibiotic Treatment Typically Last?
IV antibiotic treatment typically lasts anywhere from 7 days to 6 weeks, depending on the infection type and severity. The following sections break down standard durations for sepsis, endocarditis, osteomyelitis, meningitis, and severe pneumonia.
How Long Are IV Antibiotics Given for Sepsis?
IV antibiotics for sepsis are given for 7 to 14 days in most cases. Treatment begins immediately, often within the first hour of recognition, because delays worsen outcomes significantly. The initial course targets broad-spectrum coverage until blood cultures identify the specific pathogen. Once the organism is confirmed, clinicians narrow therapy to a targeted agent. Patients who respond well and achieve hemodynamic stability may transition to oral antibiotics before completing the full course. For sepsis caused by MRSA bloodstream infections, mortality rates between 30% and 37% have been reported by the Infectious Diseases Society of America, underscoring why aggressive early IV therapy remains standard practice.
How Long Are IV Antibiotics Given for Endocarditis?
IV antibiotics for endocarditis are given for 4 to 6 weeks, making it one of the longest standard IV antibiotic courses. Native valve endocarditis caused by streptococci may require 4 weeks, while prosthetic valve infections or staphylococcal cases often extend to 6 weeks or longer. The prolonged duration reflects how deeply bacteria embed within cardiac vegetations, where shorter courses risk relapse. Continuous bactericidal drug levels in the bloodstream are essential to sterilize these hard-to-reach sites. This is a condition where cutting treatment short carries serious consequences, including valve destruction and embolic events.
How Long Are IV Antibiotics Given for Osteomyelitis?
IV antibiotics for osteomyelitis are given for 2 to 6 weeks, depending on whether the case is acute or chronic. According to the IDSA 2021 guidelines, children with acute hematogenous osteomyelitis can often complete a short IV course followed by oral therapy, achieving outcomes comparable to prolonged intravenous regimens. Adults with chronic osteomyelitis or hardware-associated infections typically require longer IV courses. Bone tissue has limited blood supply, so sustained high antibiotic concentrations through IV delivery help penetrate infected areas more effectively. Surgical debridement frequently accompanies antibiotic therapy in chronic cases to remove necrotic bone.
How Long Are IV Antibiotics Given for Meningitis?
IV antibiotics for meningitis are given for 7 to 21 days, with duration varying by the causative organism. Neisseria meningitidis infections typically require 7 days, while Listeria monocytogenes cases may need 21 days or more. High-dose regimens are necessary because drugs must cross the blood-brain barrier to reach therapeutic concentrations in cerebrospinal fluid. According to the World Health Organization, bacterial meningitis carries approximately a 16.7% case-fatality rate, with 20% of survivors experiencing severe long-term complications. These statistics explain why aggressive, full-course IV therapy is non-negotiable for this condition.
How Long Are IV Antibiotics Given for Severe Pneumonia?
IV antibiotics for severe pneumonia are given for 7 to 14 days, though complicated cases may extend further. According to a study published in the National Library of Medicine, treatment duration for severe pneumonia cases typically averages 13.5 days. Patients hospitalized in intensive care units often receive combination IV therapy targeting both typical and atypical pathogens. Once clinical stability is achieved, including fever resolution and improved oxygenation, a step-down to oral antibiotics is standard practice. For most patients, the total antibiotic course (IV plus oral combined) falls within these timeframes unless complications such as lung abscess or empyema develop.
With treatment durations established, understanding potential side effects helps patients prepare for what to expect during therapy.
What Are the Side Effects and Risks of IV Antibiotics?
The side effects and risks of IV antibiotics range from mild injection site reactions to serious complications like organ damage and secondary infections. The following subsections cover common side effects, allergic reactions, Red Man Syndrome, organ toxicity, C. difficile risk, and IV site complications.
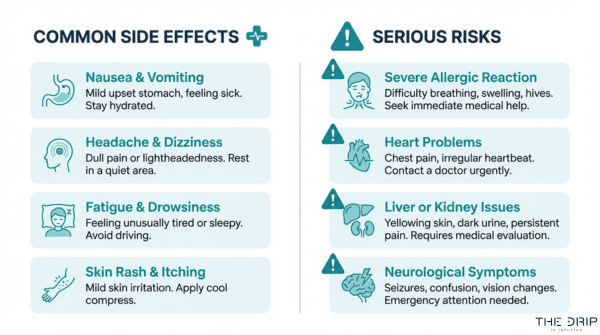
What Are the Common Side Effects of IV Antibiotics?
The common side effects of IV antibiotics include nausea, diarrhea, headache, rash, and pain or swelling at the infusion site. Gastrointestinal disturbances occur frequently because antibiotics disrupt normal gut flora alongside targeting pathogenic bacteria. Phlebitis, an inflammation of the vein used for infusion, is another regularly reported issue.
Additional common side effects include:
- Fever or chills during or shortly after infusion
- Dizziness or lightheadedness
- Metallic taste in the mouth
- Mild skin rash or flushing
- Fatigue and general malaise
Most of these reactions are self-limiting and resolve once the infusion ends or the antibiotic course is adjusted. However, any new or worsening symptom during IV antibiotic therapy warrants prompt medical evaluation.
What Allergic Reactions Can IV Antibiotics Cause?
IV antibiotics can cause allergic reactions ranging from mild skin rashes to life-threatening anaphylaxis. Beta-lactam antibiotics, including penicillins and cephalosporins, are the most common triggers. Mild reactions typically present as urticaria, itching, or localized swelling near the infusion site.
Severe allergic responses may include:
- Anaphylaxis with airway swelling, hypotension, and tachycardia
- Serum sickness with fever, joint pain, and rash appearing days after exposure
- Drug-induced interstitial nephritis
- Stevens-Johnson syndrome in rare cases
Cross-reactivity between penicillins and cephalosporins occurs in approximately 1% to 2% of patients, making allergy history essential before prescribing. For anyone with a documented beta-lactam allergy, clinicians typically select alternative classes such as vancomycin or fluoroquinolones.
What Is Red Man Syndrome From IV Vancomycin?
Red Man Syndrome from IV vancomycin is a histamine-mediated infusion reaction characterized by flushing, erythema, and pruritus of the face, neck, and upper torso. This reaction is not a true allergy; rather, it results from rapid vancomycin infusion triggering mast cell degranulation.
According to a study published in the National Library of Medicine, nephrotoxicity occurred in 18.4% of vancomycin patients, while Red Man Syndrome occurred in 2% and thrombocytopenia in 7.1% of the cohort. In pediatric populations, a retrospective study of 650 children found a 1.6% prevalence of vancomycin-induced Red Man Syndrome, with infusion rate being the most important determinant. Slowing the infusion to at least 60 minutes per gram significantly reduces occurrence, making proper administration speed critical for prevention.
Can IV Antibiotics Cause Kidney or Liver Damage?
Yes, IV antibiotics can cause kidney or liver damage, particularly with prolonged use or high-dose regimens. Nephrotoxicity is most commonly associated with vancomycin and aminoglycosides such as gentamicin, while hepatotoxicity has been linked to agents like amoxicillin-clavulanate and flucloxacillin.
Risk factors that increase organ damage potential include:
- Pre-existing renal or hepatic impairment
- Concurrent use of other nephrotoxic or hepatotoxic medications
- Extended treatment durations beyond standard protocols
- Inadequate hydration during therapy
Regular monitoring of serum creatinine, blood urea nitrogen, and liver function tests is standard practice during IV antibiotic courses. Dose adjustments based on renal clearance help minimize toxicity, which is why therapeutic drug monitoring remains essential for high-risk agents.
What Is the Risk of C. Difficile Infection With IV Antibiotics?
The risk of C. difficile infection with IV antibiotics is significant, particularly with broad-spectrum agents that severely disrupt normal gut microbiota. According to a study of 58 patients with C. difficile infection published in the National Library of Medicine, the most common antibiotic exposures were piperacillin/tazobactam (77.60%), meropenem (27.60%), and vancomycin (17.20%).
The highest-risk antibiotic classes identified by the CDC include:
- Fluoroquinolones
- Carbapenems
- Third and fourth generation cephalosporins
C. difficile produces toxins that cause watery diarrhea, abdominal cramping, and in severe cases, pseudomembranous colitis or toxic megacolon. This risk underscores why antibiotic stewardship programs emphasize using the narrowest effective spectrum for the shortest appropriate duration.
Can IV Site Complications Occur During Antibiotic Therapy?
Yes, IV site complications can occur during antibiotic therapy and represent some of the most frequent adverse events in intravenous treatment. Phlebitis, infiltration, and extravasation are the primary local complications associated with peripheral IV access.
Common IV site complications include:
- Phlebitis causing redness, warmth, and tenderness along the vein
- Infiltration where fluid leaks into surrounding tissue
- Thrombophlebitis combining vein inflammation with clot formation
- Local infection at the catheter insertion site
Certain antibiotics are particularly irritating to peripheral veins. Vancomycin and potassium-containing solutions, for instance, carry higher phlebitis risk and often require central venous access for extended courses. Routine site assessment, timely catheter rotation, and proper aseptic technique substantially reduce these complications. Understanding these risks helps patients and providers prepare for the monitoring needs that home IV antibiotic therapy demands.
Can You Receive IV Antibiotics at Home?
Yes, you can receive IV antibiotics at home through a structured medical program. The following sections cover how outpatient parenteral antibiotic therapy works, who qualifies, and what monitoring is required.
What Is Outpatient Parenteral Antibiotic Therapy?
Outpatient parenteral antibiotic therapy (OPAT) is a clinical program that allows patients to receive intravenous antibiotics outside the hospital, typically at home. OPAT enables patients with stable infections to complete their full IV antibiotic course while recovering in a familiar environment, reducing hospital stays and exposure to hospital-acquired infections.
The cost advantage is substantial. According to a 2025 study published in the National Library of Medicine, the mean cost of OPAT per episode of care is approximately $8,012, compared to $14,743 for inpatient parenteral treatment, a difference of roughly $5,437 per episode. Most OPAT programs involve a PICC line or midline catheter, with patients or trained caregivers administering scheduled doses under physician oversight. For patients facing weeks of IV antibiotic therapy, OPAT offers a practical, cost-effective alternative to prolonged hospitalization.
Who Qualifies for Home IV Antibiotic Treatment?
Patients who qualify for home IV antibiotic treatment must meet several clinical and practical criteria:
- The infection must be clinically stable, with no signs of rapid deterioration or hemodynamic instability.
- The patient must have reliable venous access, such as a PICC line, that can remain functional for the full treatment duration.
- A safe, clean home environment with adequate refrigeration for medication storage is required.
- The patient or a caregiver must demonstrate competency in operating the infusion equipment and recognizing warning signs.
- The prescribing physician must confirm that the chosen antibiotic is appropriate for home administration, with a manageable dosing schedule.
Patients with uncontrolled comorbidities, active substance use disorders, or limited support systems may not be appropriate candidates. The final determination always involves the treating infectious disease specialist or physician.
What Monitoring Is Needed During Home IV Antibiotics?
Monitoring during home IV antibiotics includes regular clinical assessments and laboratory testing to ensure treatment safety and efficacy. Key monitoring requirements are:
- Blood work: Periodic complete blood counts, renal function panels, and drug levels (particularly for vancomycin or aminoglycosides) are drawn at scheduled intervals.
- IV site inspection: The catheter insertion site must be checked daily for redness, swelling, tenderness, or drainage that could indicate infection.
- Clinical response tracking: Temperature, symptom progression, and overall functional status are documented and reported to the supervising physician.
- Adverse reaction surveillance: Patients must know when to seek emergency care, including signs of allergic reaction, severe diarrhea suggesting C. difficile, or sudden changes in urine output.
Most OPAT programs schedule weekly or biweekly in-person or telehealth visits with the care team. With proper monitoring protocols, home IV antibiotic therapy maintains safety standards comparable to inpatient care while supporting faster return to daily life.
How Do IV Antibiotics Relate to Antibiotic Resistance?
IV antibiotics relate to antibiotic resistance through both their potential to drive resistant bacterial strains and their role in stewardship programs designed to limit unnecessary use.
Broad-spectrum IV antibiotics, when prescribed without targeted culture data, expose bacteria to selective pressure that favors resistant mutations. Each unnecessary course increases the likelihood that surviving organisms develop mechanisms to evade treatment. Overuse of empiric IV therapy in hospital settings accelerates this cycle, particularly with agents active against gram-negative pathogens.
According to the Centers for Disease Control and Prevention, more than 2.8 million antimicrobial-resistant infections occur each year in the United States, resulting in more than 35,000 deaths, with an estimated national cost exceeding $4.6 billion annually to treat infections caused by six common resistant germs.
Antibiotic stewardship programs directly address this problem by promoting several key practices:
- Narrowing IV antibiotic coverage once culture and sensitivity results are available.
- Transitioning patients from IV to oral therapy as soon as clinical criteria are met.
- Shortening IV treatment durations based on evidence-based guidelines rather than tradition.
- Avoiding broad-spectrum agents when narrower-spectrum options are effective.
The connection between IV antibiotics and resistance is not about the route itself; it is about how and when these powerful agents are used. Poorly targeted IV therapy selects for resistant organisms, while disciplined prescribing preserves antibiotic effectiveness for future patients. This distinction matters because resistance does not reverse easily once it becomes established in a bacterial population.
For anyone receiving IV antibiotics, understanding why stewardship matters reinforces the importance of following prescribed courses exactly as directed. Knowing what to discuss with your doctor before starting treatment helps ensure the right antibiotic is selected from the outset.
What Should You Ask Your Doctor Before Starting IV Antibiotics?
You should ask your doctor about the specific infection being treated, expected treatment duration, potential side effects, and whether oral alternatives exist. The questions below cover the most important topics to discuss before beginning intravenous antibiotic therapy.
- What infection am I being treated for, and which organism was identified? Understanding the specific pathogen guides antibiotic selection and helps you follow the rationale behind your treatment plan.
- Why is IV administration necessary instead of oral antibiotics? Some antibiotics, such as metronidazole and fluconazole, have oral bioavailability exceeding 90%, so clarifying the clinical need for intravenous delivery is reasonable.
- How long will treatment last, and when can I switch to oral therapy? Duration varies significantly by condition; asking about step-down criteria helps set realistic expectations.
- What side effects should I watch for? Each antibiotic class carries distinct risks, from nephrotoxicity with vancomycin to gastrointestinal disruption with broad-spectrum agents.
- What is my risk for C. difficile infection? According to a study published in the National Library of Medicine (PMC), the highest-risk antibiotic classes for C. difficile include fluoroquinolones, carbapenems, and third/fourth-generation cephalosporins.
- Can I receive treatment at home through OPAT? Not every patient qualifies, so discussing eligibility for outpatient parenteral therapy early can influence your care plan.
- Will any lab work or monitoring be needed during treatment? Kidney function tests, drug levels, and blood counts are commonly required depending on the antibiotic prescribed.
Patients who ask these questions gain clearer expectations and become more active participants in their care. With a solid understanding of your IV antibiotic plan, exploring complementary support strategies becomes a natural next step.
How Can IV Therapy Support Your Recovery Alongside Treatment?
IV therapy can support your recovery alongside treatment by delivering hydration, vitamins, and immune-boosting nutrients directly into the bloodstream while you follow your prescribed medical plan. The following sections cover mobile IV support during illness and key takeaways about IV antibiotics.
Can Mobile IV Hydration and Immune Support Help During Illness?
Yes, mobile IV hydration and immune support can help during illness by restoring fluid balance and delivering nutrients that support immune function without requiring a hospital visit. Staying well-hydrated is essential when the body fights infection, and IV delivery ensures maximum absorption by bypassing the GI tract.
Adjunctive IV therapies have been studied in clinical settings. According to a systematic review published in the National Library of Medicine (PMC), intravenous high-dose vitamin C monotherapy in sepsis patients showed mixed results; some reviews suggest modest physiological benefits and potential improvement in short-term mortality, while one major trial indicated potential harm in terms of persistent organ dysfunction.
These findings underscore an important distinction: wellness-focused IV hydration with vitamins like vitamin C, zinc, and B-complex differs from high-dose clinical protocols used in critical care. For individuals recovering from common illnesses, a mobile IV session focused on hydration and moderate immune support can complement prescribed treatments without replacing them. The Drip IV Infusion offers mobile IV hydration and immune support infusions with add-ons such as vitamin C, zinc, and glutathione, delivered by experienced nurses in the comfort of your home.
What Are the Key Takeaways About IV Antibiotics?
The key takeaways about IV antibiotics are that they serve as a critical tool for treating severe infections, but their use requires careful clinical oversight and awareness of both benefits and risks.
- IV antibiotics deliver 100% bioavailability, making them essential when oral therapy cannot achieve adequate drug levels.
- Conditions such as sepsis, bacterial meningitis, endocarditis, and osteomyelitis frequently require intravenous antibiotic administration.
- Side effects range from infusion site reactions and allergic responses to serious complications like nephrotoxicity and C. difficile infection.
- Outpatient parenteral antibiotic therapy (OPAT) allows eligible patients to continue IV antibiotics at home at significantly lower cost than inpatient care.
- Antibiotic resistance remains a growing concern; responsible stewardship and appropriate IV-to-oral switching help preserve antibiotic effectiveness.
- Supportive hydration and immune-focused IV therapy can complement your recovery plan but should never replace prescribed antibiotic treatment.
Always discuss your treatment options, potential side effects, and transition plans with your healthcare provider before starting or stopping IV antibiotics. For supportive IV hydration and immune wellness alongside your medical care, The Drip IV Infusion provides personalized mobile infusions tailored to your recovery needs.